University of Winchester, Winchester, UK.
Hampshire Hospitals NHS Foundation Trust, Basingstoke, UK.
Am J Sports Med. 2021 Apr;49(5):1372-1380. doi: 10.1177/0363546520948861. Epub 2020 Sep 22.
The 2 most common definitive surgical interventions currently performed for the treatment of medial osteoarthritis of the knee are medial opening wedge high tibial osteotomy (HTO) and medial unicompartmental knee arthroplasty (UKA). Research exists to suggest that physically active patients may be suitably indicated for either procedure despite HTO being historically indicated in active patients and UKA being more appropriate for sedentary individuals.
To help consolidate the current indications for both procedures regarding physical activity and to ensure that they are based on the best information presently available.
Systematic review.
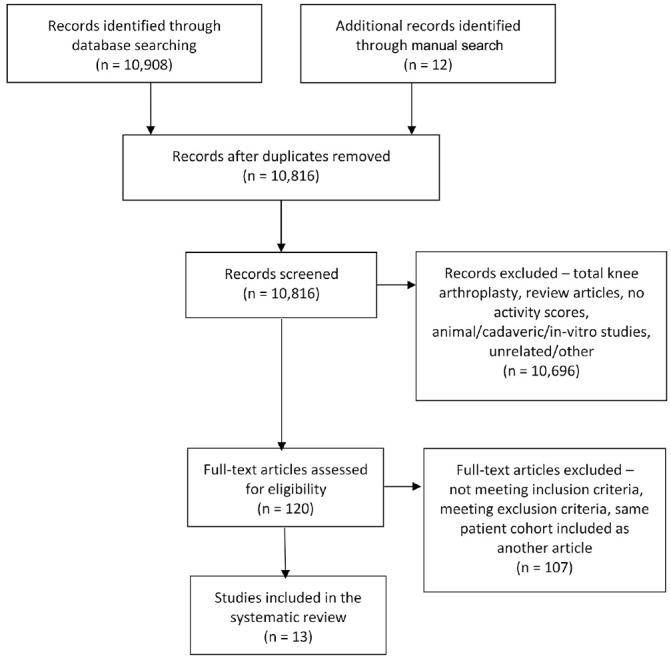
A search of the literature via the MEDLINE, Embase, and PubMed databases was conducted independently by 2 reviewers in accordance with the PRISMA (Preferred Reporting Items for Systematic Meta-Analyses) guidelines. Studies that reported patient physical activity levels with the Tegner activity score were eligible for inclusion. Patient demographics, operative variables, and patient-reported outcome scores were abstracted from the included studies.
Thirteen eligible studies were included, consisting of 401 knees that received HTO (399 patients) and 1622 that received UKA (1400 patients). The patients' mean age at surgery was 48.4 years for the HTO group and 60.6 years for the UKA group. Mean follow-up was 46.6 months (HTO) and 53.4 months (UKA). All outcome scores demonstrated an equal or improved score for activity and knee function regardless of the operation performed. Operative variables during HTO had a larger effect on outcome than during UKA.
Patients who underwent HTO were more physically active pre- and postoperatively, but patients undergoing UKA experienced an overall greater increase in their physical activity levels and knee function according to Tegner and Lysholm scores. Activity after HTO may be influenced by operative factors such as the implant used and the decision to include a graft material in the osteotomy gap, although this requires further research. Some studies found that patients were able to return to physical activity postoperatively despite having an age or body mass index that would traditionally be a relative contraindication for HTO or UKA.
目前治疗膝关节内侧骨关节炎的两种最常见的确定性手术干预方法是内侧开放楔形胫骨高位截骨术(HTO)和内侧单髁膝关节置换术(UKA)。有研究表明,尽管 HTO 历史上适用于活跃患者,而 UKA 更适用于久坐的个体,但对于活跃患者,两种手术方法都可能是合适的选择。
帮助整合这两种手术方法的当前活动水平适应证,并确保这些适应证基于目前可获得的最佳信息。
系统评价。
两名评审员按照 PRISMA(系统评价和荟萃分析的首选报告项目)指南通过 MEDLINE、Embase 和 PubMed 数据库进行文献检索。符合纳入标准的研究报告了患者的体力活动水平和 Tegner 活动评分。从纳入的研究中提取患者的人口统计学、手术变量和患者报告的结果评分。
共纳入 13 项符合条件的研究,其中 401 例膝关节接受 HTO(399 例患者),1622 例膝关节接受 UKA(1400 例患者)。HTO 组患者的平均手术年龄为 48.4 岁,UKA 组为 60.6 岁。HTO 的平均随访时间为 46.6 个月,UKA 为 53.4 个月。无论进行哪种手术,所有的结果评分都显示活动和膝关节功能的评分相等或提高。HTO 术中的手术变量对结果的影响大于 UKA。
接受 HTO 的患者术前和术后的体力活动水平更高,但根据 Tegner 和 Lysholm 评分,接受 UKA 的患者的体力活动水平和膝关节功能总体上有更大的提高。HTO 术后的活动水平可能受到手术因素的影响,例如使用的植入物和决定在截骨间隙中加入移植物材料,但这需要进一步的研究。一些研究发现,尽管患者的年龄或体重指数传统上是 HTO 或 UKA 的相对禁忌症,但他们仍能在术后恢复体力活动。