Department of Radiation Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100021, China.
Department 4th of Radiation Oncology, Anyang Cancer Hospital, Anyang, 455000, China.
BMC Cancer. 2020 Sep 22;20(1):901. doi: 10.1186/s12885-020-07387-y.
Since the development of three-dimensional conformal radiotherapy and intensity-modulated radiotherapy (IMRT), no prospective study has investigated whether concurrent chemoradiotherapy (SIB-IMRT with 60 Gy) remains superior to radiotherapy (SIB-IMRT) alone for unresectable esophageal cancer (EC). Furthermore, the optimal therapeutic regimen for patients who cannot tolerate concurrent chemoradiotherapy is unclear. We recently completed a phase I/II radiation dose-escalation trial using simultaneous integrated boost (SIB), elective nodal irradiation, and concurrent chemotherapy for unresectable EC. We now intend to conduct a prospective, phase III, randomized study of SIB-IMRT with or without concurrent chemotherapy. We aim to find a safe, practical, and effective therapeutic regimen to replace the conventional segmentation (1.8-2.0 Gy) treatment mode (radiotherapy ± chemotherapy) for unresectable EC.
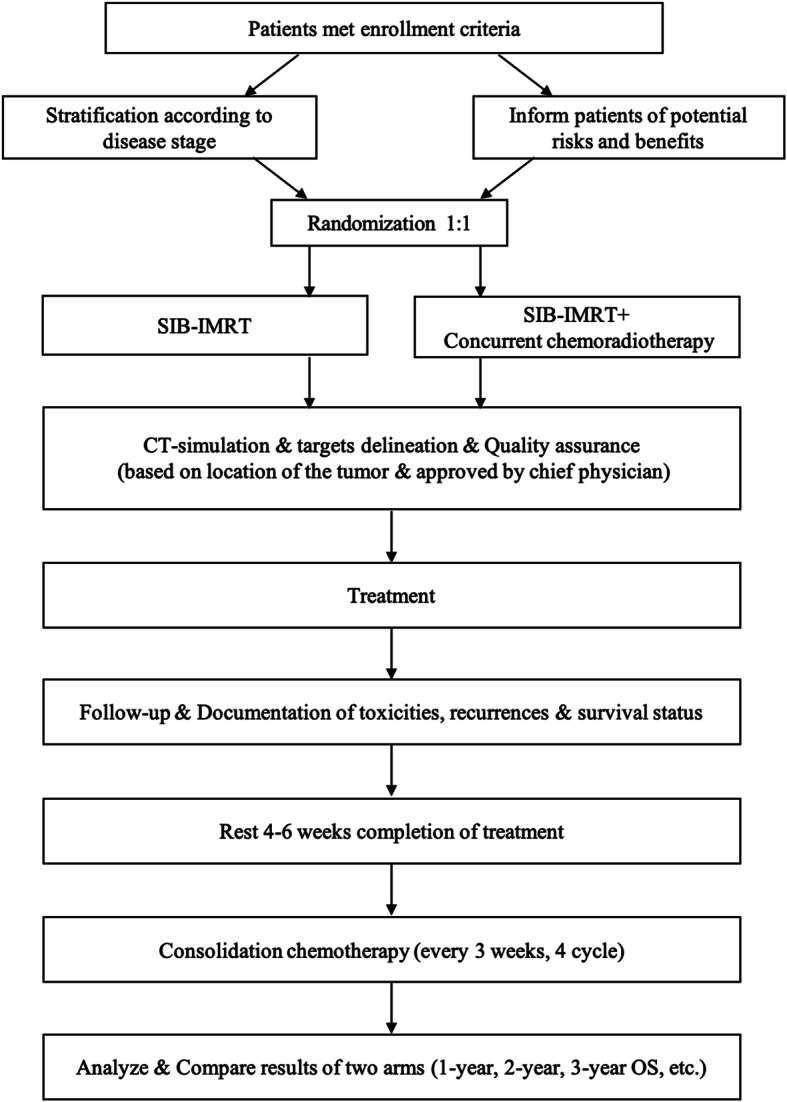
This two-arm, open, randomized, multicenter, phase III trial will recruit esophageal squamous cell carcinoma patients (stage IIA-IVB [UICC 2002]; IVB only with metastasis to the supraclavicular or celiac lymph nodes). In all, 164 patients will be randomized using a 1:1 allocation ratio, and stratified by study site and disease stage, especially the extent of lymph node metastasis. Patients in the SIB arm will receive definitive SIB radiotherapy (95% planning target volume/planning gross tumor volume, 50.4 Gy/59.92 Gy/28 f, equivalent dose in 2-Gy fractions = 60.62 Gy). Patients in the SIB + concurrent chemotherapy arm will receive definitive SIB radiotherapy with weekly paclitaxel and a platinum-based drug (5-6 weeks). Four cycles of consolidated chemoradiotherapy will also be recommended. The primary objective is to compare the 1-year, 2-year, and 3-year overall survival of the SIB + chemotherapy group and SIB groups. Secondary objectives include progression-free survival, local recurrence-free rate, completion rate, and adverse events. Detailed radiotherapy protocol and quality-assurance procedures have been incorporated into this trial.
In unresectable, locally advanced EC, a safe and effective total radiotherapy dose and reasonable segmentation doses are required for the clinical application of SIB-IMRT + two-drug chemotherapy. Whether this protocol will replace the standard treatment regimen will be prospectively investigated. The effects of SIB-IMRT in patients with poor physical condition who cannot tolerate definitive chemoradiotherapy will also be investigated.
clinicaltrials.gov ( NCT03308552 , November 1, 2017).
自三维适形放疗和调强放疗(IMRT)发展以来,尚无前瞻性研究表明不可切除食管癌(EC)的同步放化疗(SIB-IMRT 联合 60Gy)是否仍优于单纯放疗(SIB-IMRT)。此外,对于不能耐受同步放化疗的患者,最佳治疗方案尚不清楚。我们最近完成了一项使用同步整合推量(SIB)、选择性淋巴结照射和同步化疗治疗不可切除 EC 的 I/II 期放疗剂量递增试验。我们现在打算进行一项前瞻性、III 期、随机研究,比较 SIB-IMRT 联合或不联合同步化疗的效果。我们旨在寻找一种安全、实用、有效的治疗方案,以替代常规分割(1.8-2.0Gy)治疗模式(放疗±化疗)治疗不可切除的 EC。
这项两臂、开放、随机、多中心、III 期试验将招募食管鳞状细胞癌患者(IIA-IVB 期[UICC 2002];IVB 期仅伴锁骨上或腹腔淋巴结转移)。共 164 例患者将采用 1:1 分配比例随机分组,并按研究地点和疾病分期分层,尤其是淋巴结转移程度。SIB 组患者将接受根治性 SIB 放疗(95%计划靶区/计划大体肿瘤靶区,50.4Gy/59.92Gy/28f,2Gy 等效剂量=60.62Gy)。SIB+同期化疗组患者将接受根治性 SIB 放疗联合每周紫杉醇和铂类药物(5-6 周)。还建议进行 4 个周期的巩固放化疗。主要终点是比较 SIB+化疗组和 SIB 组的 1 年、2 年和 3 年总生存率。次要终点包括无进展生存期、局部无复发生存率、完成率和不良事件。详细的放疗方案和质量保证程序已纳入本试验。
对于不可切除的局部晚期 EC,需要 SIB-IMRT+两药化疗的安全有效总放疗剂量和合理分割剂量,以便于 SIB-IMRT 的临床应用。该方案是否会替代标准治疗方案将前瞻性地进行研究。还将研究 SIB-IMRT 对不能耐受根治性放化疗的身体状况不佳患者的效果。
clinicaltrials.gov(NCT03308552,2017 年 11 月 1 日)。