Kallianpur Kalpana J, Birn Rasmus, Ndhlovu Lishomwa C, Souza Scott A, Mitchell Brooks, Paul Robert, Chow Dominic C, Kohorn Lindsay, Shikuma Cecilia M
Department of Tropical Medicine, Medical Microbiology and Pharmacology, University of Hawaii-Manoa, Honolulu, HI, USA.
Center for Translational Research on Aging, Kuakini Medical Center, Honolulu, HI, USA.
J Behav Brain Sci. 2020 Aug;10(8):344-370. Epub 2020 Aug 21.
Brain atrophy and cognitive deficits persist among individuals with suppressed HIV disease. The impact of cannabis use is unknown.
HIV+ and HIV- participants underwent cross-sectional magnetic resonance imaging and neuropsychological testing. Lifetime frequency, duration (years), and recency of cannabis use were self-reported. Relationships of cannabis use to resting-state functional connectivity (RSFC) and to 9 regional brain volumes were assessed with corrections for multiple comparisons. Peripheral blood cytokines and monocyte subsets were measured in the HIV+ group and examined in relation to cannabis exposure.
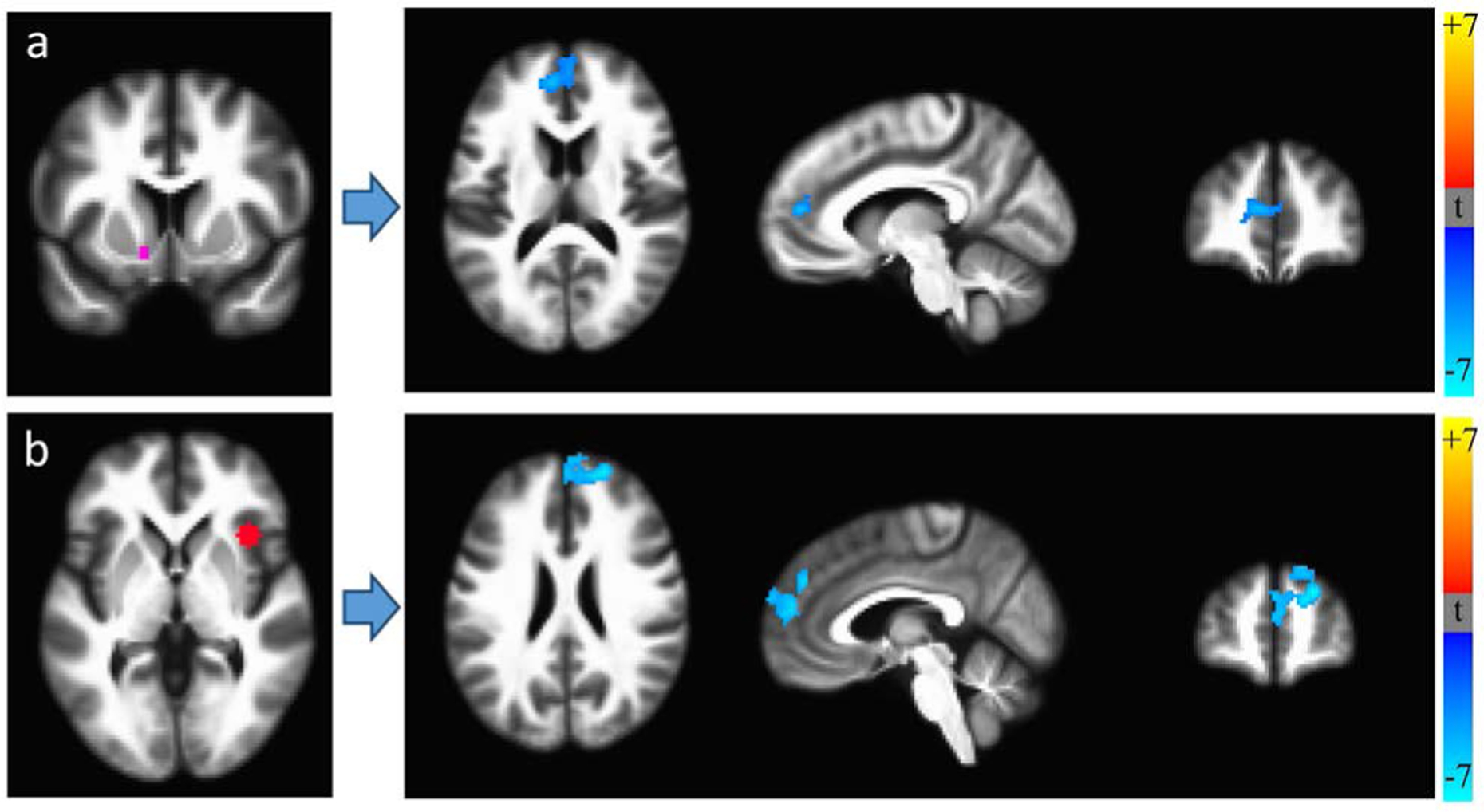
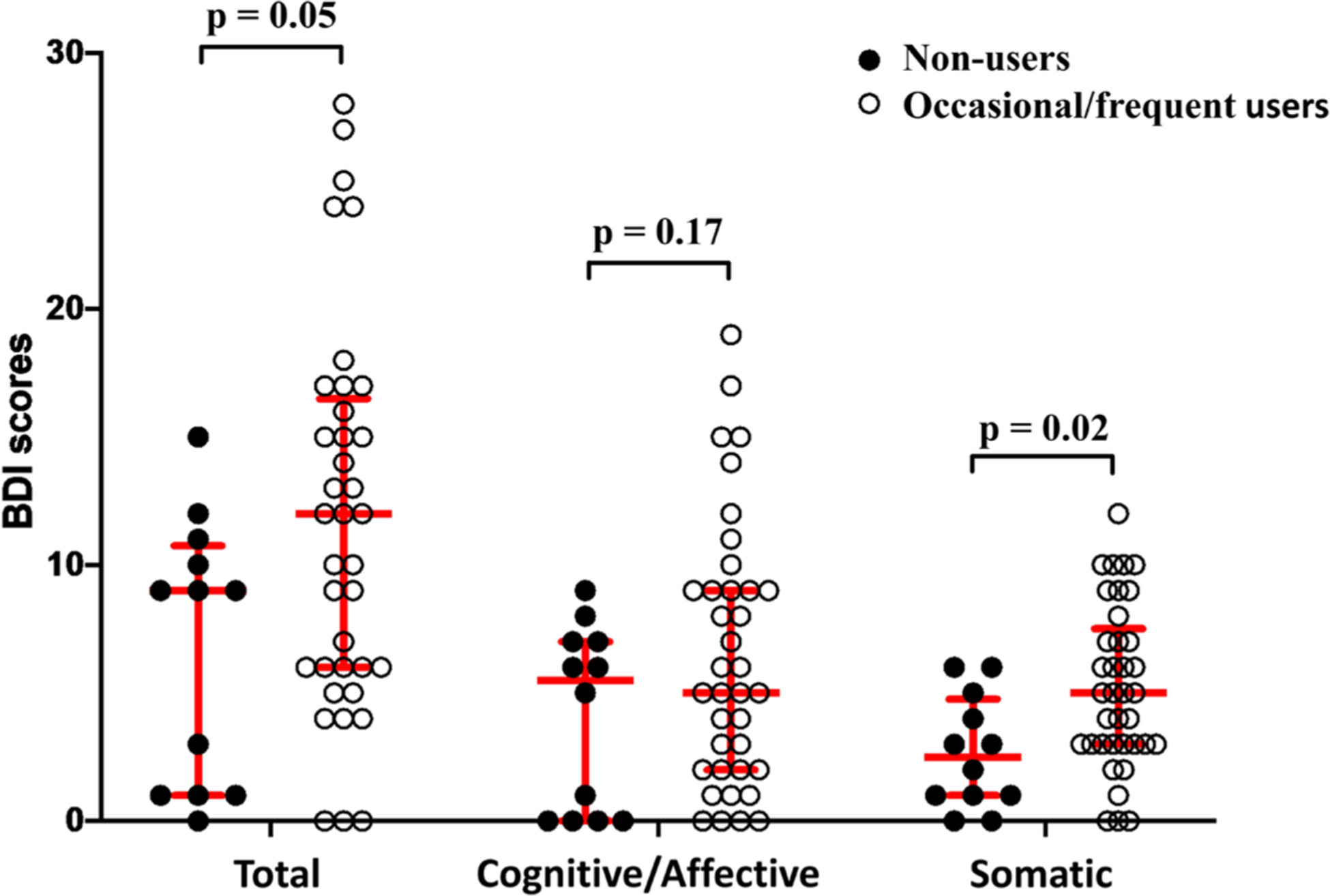
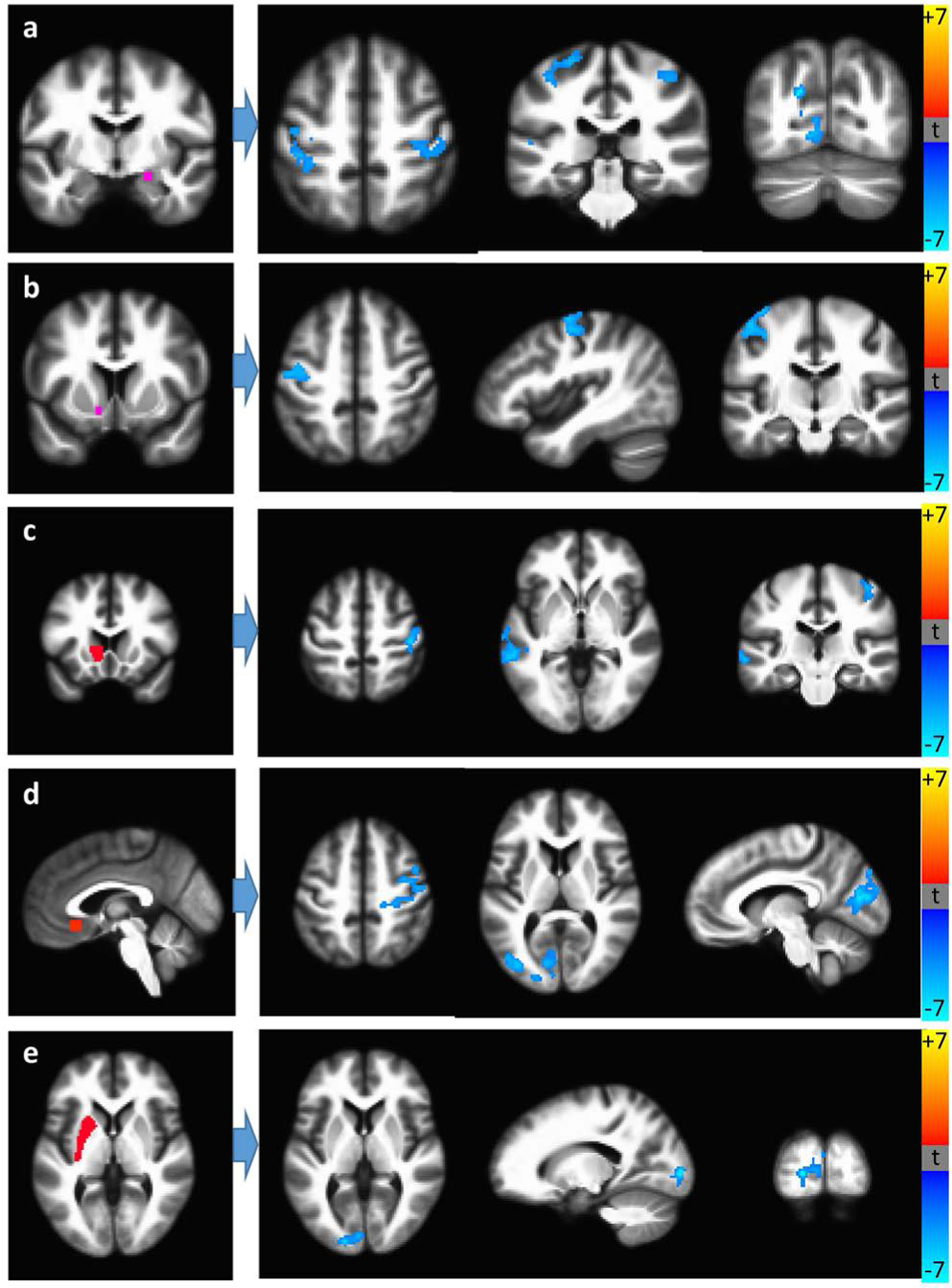
We evaluated 52 HIV+ [50.8 ± 7.1 years old; 100% on antiretroviral therapy ≥ 3 months; 83% with plasma viral load < 50 copies/mL] and 55 HIV- [54.0 ± 7.5 years old] individuals. Among HIV+ participants, recent cannabis use (within 12 months) was associated with diminished RSFC, including of occipital cortex, controlling for age. Duration of use correlated negatively with volumes of all regions (most strikingly the nucleus accumbens) independently of recent use and intracranial volume. Recent use was associated with larger caudate and white matter volumes and lower soluble vascular cell adhesion molecule-1 and monocyte chemoattractant protein-1 concentrations. Duration of use correlated positively with psychomotor speed. Use > 10 times/lifetime was linked to more somatic symptoms, better executive function, and lower CD14CD16 monocyte count.
HIV+ individuals demonstrated opposing associations with cannabis. Recent use may weaken RSFC and prolonged consumption may exacerbate atrophy of the accumbens and other brain regions. More frequent or recent cannabis use may reduce the inflammation and CD14CD16 monocytes that facilitate HIV neuroinvasion. HIV-specific cannabis studies are necessary.
在HIV疾病得到抑制的个体中,脑萎缩和认知缺陷仍然存在。大麻使用的影响尚不清楚。
HIV阳性和HIV阴性参与者接受了横断面磁共振成像和神经心理学测试。通过自我报告了解大麻使用的终生频率、持续时间(年)和近期使用情况。在进行多重比较校正后,评估大麻使用与静息态功能连接(RSFC)以及9个脑区体积之间的关系。在HIV阳性组中测量外周血细胞因子和单核细胞亚群,并检查其与大麻暴露的关系。
我们评估了52名HIV阳性个体[年龄50.8±7.1岁;100%接受抗逆转录病毒治疗≥3个月;83%血浆病毒载量<50拷贝/mL]和55名HIV阴性个体[年龄54.0±7.5岁]。在HIV阳性参与者中,近期使用大麻(在12个月内)与RSFC降低有关,包括枕叶皮质,校正了年龄因素。使用持续时间与所有区域的体积呈负相关(最显著的是伏隔核),与近期使用情况和颅内体积无关。近期使用与尾状核和白质体积增大以及可溶性血管细胞黏附分子-1和单核细胞趋化蛋白-1浓度降低有关。使用持续时间与精神运动速度呈正相关。终生使用>10次与更多躯体症状、更好的执行功能和更低的CD14CD16单核细胞计数有关。
HIV阳性个体与大麻存在相反的关联。近期使用可能会削弱RSFC,长期使用可能会加剧伏隔核和其他脑区的萎缩。更频繁或近期使用大麻可能会减少促进HIV神经侵袭的炎症和CD14CD16单核细胞。有必要开展针对HIV患者的大麻研究。