Division of Physical Medicine & Rehabilitation, University of Utah, Salt Lake City, UT.
Department of Physical Medicine & Rehabilitation, University of Texas Health Science Center, San Antonio, TX.
PM R. 2021 Sep;13(9):962-968. doi: 10.1002/pmrj.12499. Epub 2020 Nov 23.
Physician decision-making surrounding choices for large joint and bursa injections is poorly defined, yet influences patient safety and treatment effectiveness.
To identify practice patterns and rationale related to injectate choices for large joint and bursal injections performed by physician members of the American Medical Society for Sports Medicine (AMSSM).
An electronic survey was sent to 3400 members of the AMSSM. Demographic variables were collected: primary specialty (residency), training location, practice location, years of clinical experience, current practice type, and rationale for choosing an injectate.
A total of 674 physicians responded (minimum response rate of 20%).
Not applicable.
Outcomes of interest included corticosteroid type and dose, local anesthetic type, and total injectate volume for each large joint or bursa (hip, knee, and shoulder).
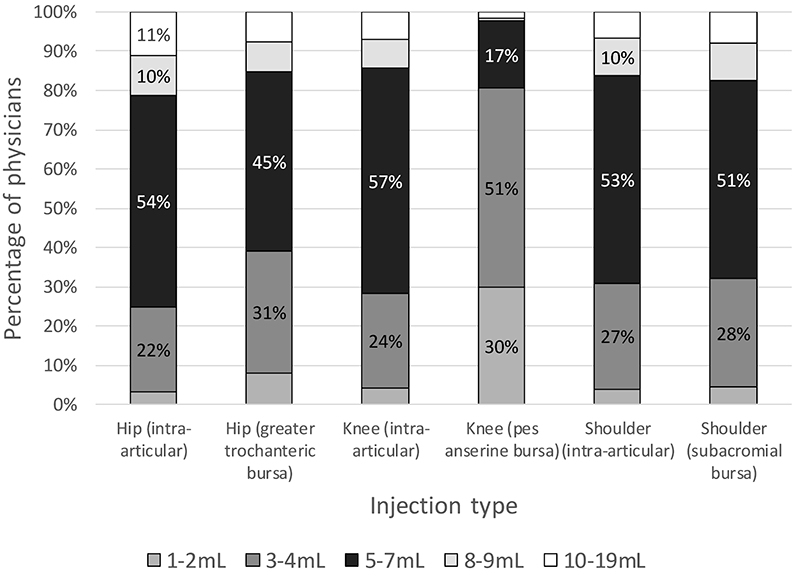
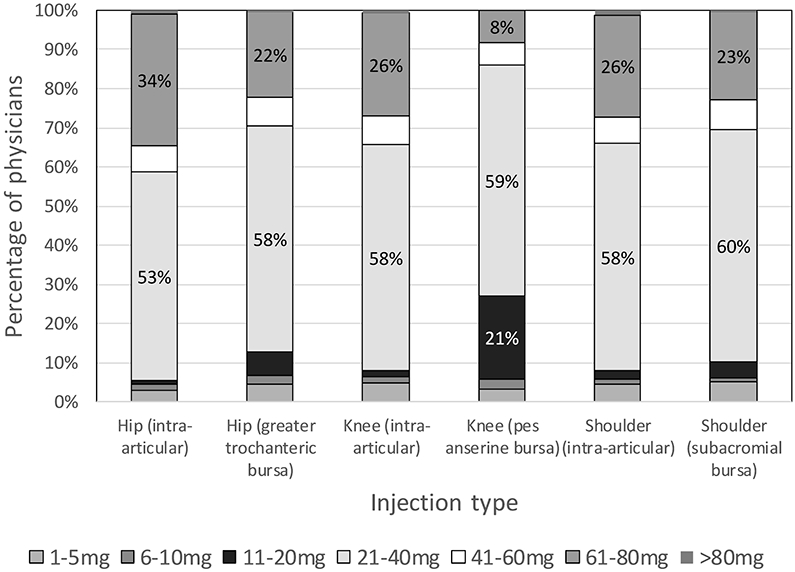
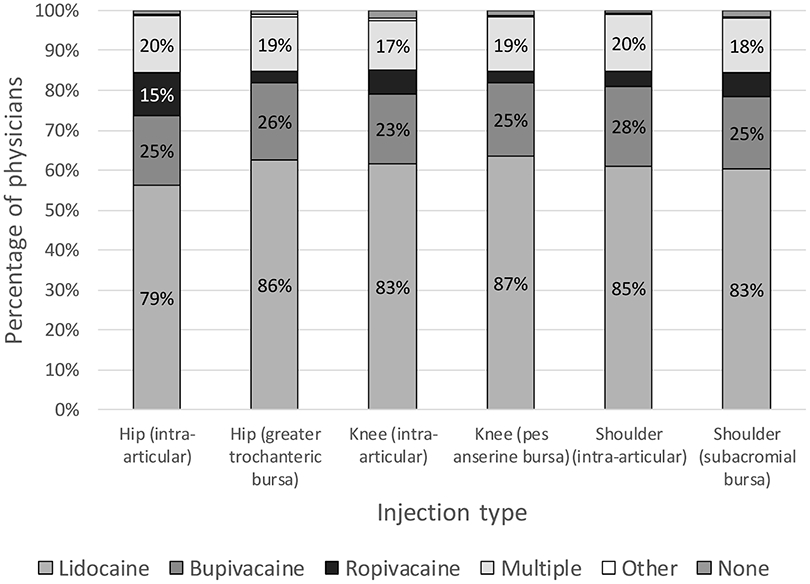
Most respondents used triamcinolone (50% to 56% of physicians, depending on injection location) or methylprednisolone (25% to 29% of physicians), 21 to 40 mg (53% to 60% of physicians), diluted with lidocaine (79% to 87%) for all large joint or bursa injections. It was noted that 36.2% (244/674) of respondents reported using >40 mg for at least one injection type. Most (90.5%, 610/674) reported using an anesthetic other than ropivacaine for at least one type of joint or bursa injection. Physicians who reported lidocaine use were less likely to report that their injectate choice was based on the literature that they reviewed (odds ratio [OR] 0.41 [0.27-0.62], P < .001). Respondents predominantly used 5 to 7 mL of total injectate for all large joints or bursae (45% to 54% of respondents), except for the pes anserine bursa, where 3-4 mL was more common (51% of physicians).
It appears that triamcinolone and methylprednisolone are the most commonly used corticosteroids for sports medicine physicians; most physicians use 21 to 40 mg of corticosteroid for all injections, and lidocaine is the most-often used local anesthetic; very few use ropivacaine. Over one-third of respondents used high-dose (>40 mg triamcinolone or methylprednisolone) for at least one joint or bursa.
美国运动医学学会(AMSSM)的医师在选择大关节和滑囊注射时,其决策方法并不明确,但会影响患者的安全和治疗效果。
确定 AMSSM 医师进行大关节和滑囊注射时选择注射剂的实践模式和原理。
向 AMSSM 的 3400 名成员发送了电子调查。收集了人口统计学变量:主要专业(住院医师)、培训地点、实践地点、临床经验年限、当前实践类型以及选择注射剂的原理。
共有 674 名医生做出了回应(最低回应率为 20%)。
不适用。
感兴趣的结果包括每个大关节或滑囊(髋、膝和肩)的皮质类固醇类型和剂量、局部麻醉剂类型和总注射量。
大多数受访者使用曲安奈德(50%至 56%的医生,取决于注射部位)或甲泼尼龙(25%至 29%的医生),21 至 40mg(53%至 60%的医生),用利多卡因稀释(79%至 87%)用于所有大关节或滑囊注射。值得注意的是,36.2%(244/674)的受访者报告说至少有一种注射类型使用了>40mg。大多数(90.5%,610/674)报告至少有一种关节或滑囊注射使用了除罗哌卡因以外的麻醉剂。报告使用利多卡因的医生不太可能表示他们的注射剂选择是基于他们审查的文献(优势比[OR]0.41[0.27-0.62],P<.001)。受访者主要使用 5 至 7ml 的总注射量用于所有大关节或滑囊(45%至 54%的受访者),除了鹅足滑囊炎,其中 3 至 4ml 更为常见(51%的医生)。
曲安奈德和甲泼尼龙似乎是运动医学医师最常使用的皮质类固醇;大多数医生对所有注射使用 21 至 40mg 的皮质类固醇,利多卡因是最常使用的局部麻醉剂;很少使用罗哌卡因。超过三分之一的受访者至少有一种关节或滑囊使用了高剂量(>40mg 曲安奈德或甲泼尼龙)。