Wan Xiang-Bo, Zhang Qun, Chen Mo, Liu Yanping, Zheng Jian, Lan Ping, He Fang
Department of Radiation Oncology, The Sixth Affiliated Hospital of Sun Yat-sen University, Guangzhou, China.
Department of Radiation Oncology, The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, China.
Front Oncol. 2020 Aug 21;10:1280. doi: 10.3389/fonc.2020.01280. eCollection 2020.
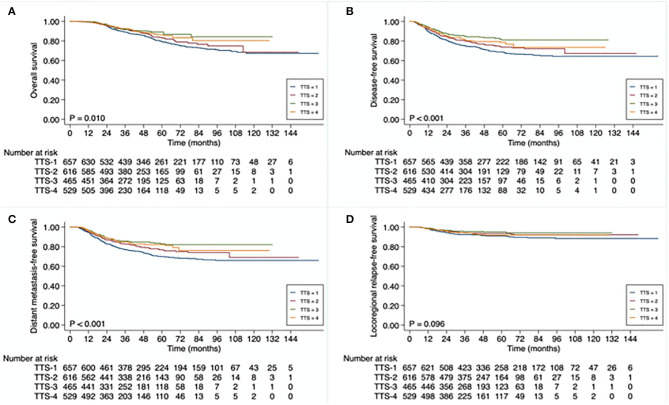
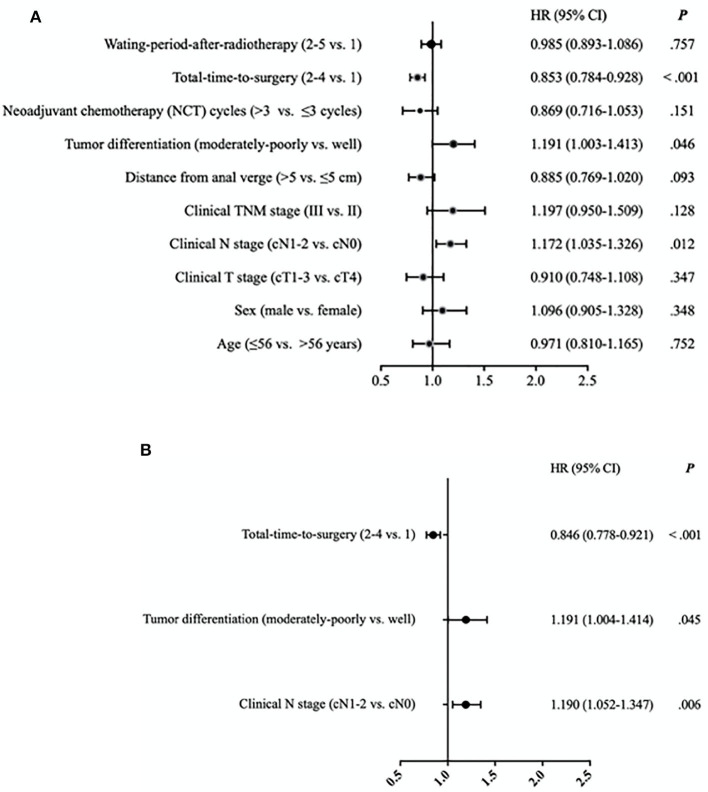
The addition of intensive preoperative chemotherapy and using of a longer waiting period between neoadjuvant radiotherapy and total mesorectal excision (TME) surgery lengthen the time interval from the initiation of neoadjuvant treatment to definitive surgery in patients with locally advanced rectal cancer (LARC). Here, we evaluated the prognostic value of different time intervals between the initiation of neoadjuvant treatment to TME surgery for LARC. A total of 2,267 patients with LARC, who received neoadjuvant radiochemotherapy and TME surgery, between January 2010 through December 2018 were recruited. The entire cohort was divided into 4 subgroups based on total-time-to surgery, defined as the time interval between initiation of neoadjuvant treatment and TME surgery (TTS): <13 weeks (TTS-1), 13 to <15 weeks (TTS-2), 15 to <17 weeks (TTS-3), ≥17 weeks (TTS-4). Overall survival (OS), disease-free survival (DFS), distant metastasis-free survival (DMFS), and local recurrence-free survival (LRFS) rates in different TTS subgroup patients were compared, and hazard ratios (HR) for different demographic and clinicopathological variables, including TTS, were calculated to determine their prognostic significance. The median follow-up time was 42.0 (range, 5-162) months. The 3-year OS, DFS, DMFS, and LRFS rates were 87.0, 79.4, 80.9, and 93.8%, respectively. The varied OS, DFS, and DFMS rates were detected among these different TTS subgroups ( = 0.010, < 0.001, and < 0.001, respectively). Particularly, the lower survival outcome was mainly observed at patients in the shortest TTS group (TTS-1). Cox regression analysis confirmed that the only significant positive independent prognostic factor for 3-year DFS was a longer TTS (TTS 2-4 vs. TTS-1; HR 0.884, 95% CI 0.778-0.921, < 0.001), while the significant negative independent prognosticfactors were moderate to poor tumor differentiation (vs. well-differentiated; HR 1.191, 95% CI 1.004-1.414, = 0.045) and clinical N1-2 stage (vs. N0 stage; HR 1.190, 95% CI 1.052-1.347, = 0.006). For patients with LARC, an interval between the initiation of neoadjuvant treatment and TME surgery of longer than 13 weeks is associated with favorable disease-free survival.
强化术前化疗的加入以及在新辅助放疗和全直肠系膜切除术(TME)手术之间采用更长的等待期,延长了局部晚期直肠癌(LARC)患者从新辅助治疗开始到确定性手术的时间间隔。在此,我们评估了新辅助治疗开始至LARC患者进行TME手术之间不同时间间隔的预后价值。招募了2010年1月至2018年12月期间共2267例接受新辅助放化疗和TME手术的LARC患者。整个队列根据手术总时间分为4个亚组,手术总时间定义为新辅助治疗开始至TME手术的时间间隔(TTS):<13周(TTS-1)、13至<15周(TTS-2)、15至<17周(TTS-3)、≥17周(TTS-4)。比较了不同TTS亚组患者的总生存期(OS)、无病生存期(DFS)、无远处转移生存期(DMFS)和无局部复发生存期(LRFS)率,并计算了包括TTS在内的不同人口统计学和临床病理变量的风险比(HR),以确定其预后意义。中位随访时间为42.0(范围5-162)个月。3年OS、DFS、DMFS和LRFS率分别为87.0%、79.4%、80.9%和93.8%。在这些不同的TTS亚组中检测到了不同的OS、DFS和DFMS率(分别为=0.010、<0.001和<0.001)。特别是,在最短TTS组(TTS-1)的患者中主要观察到较低的生存结果。Cox回归分析证实,3年DFS的唯一显著正独立预后因素是更长的TTS(TTS 2-4与TTS-1相比;HR 0.884,95%CI 0.778-0.921,<0.001),而显著负独立预后因素是中度至差的肿瘤分化(与高分化相比;HR 1.191,95%CI 1.004-1.414,=0.045)和临床N1-2期(与N0期相比;HR 1.190,95%CI 1.052-1.347,=0.006)。对于LARC患者,新辅助治疗开始至TME手术之间超过13周的时间间隔与良好的无病生存相关。