William Harvey Research Institute, Barts and The London School of Medicine and Dentistry, Queen Mary University of London, London, UK.
Critical Care and Perioperative Medicine Research Group, Adult Critical Care Unit, Royal London Hospital, London, E1 1BB, UK.
Crit Care. 2020 Sep 25;24(1):577. doi: 10.1186/s13054-020-03275-w.
Patients who survive critical illness suffer from a significant physical disability. The impact of rehabilitation strategies on health-related quality of life is inconsistent, with population heterogeneity cited as one potential confounder. This secondary analysis aimed to (1) examine trajectories of functional recovery in critically ill patients to delineate sub-phenotypes and (2) to assess differences between these cohorts in both clinical characteristics and clinimetric properties of physical function assessment tools.
Two hundred ninety-one adult sepsis survivors were followed-up for 24 months by telephone interviews. Physical function was assessed using the Physical Component Score (PCS) of the Short Form-36 Questionnaire (SF-36) and Activities of Daily Living and the Extra Short Musculoskeletal Function Assessment (XSFMA-F/B). Longitudinal trajectories were clustered by factor analysis. Logistical regression analyses were applied to patient characteristics potentially determining cluster allocation. Responsiveness, floor and ceiling effects and concurrent validity were assessed within clusters.
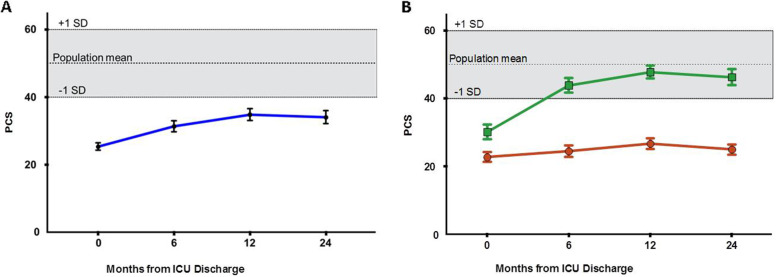
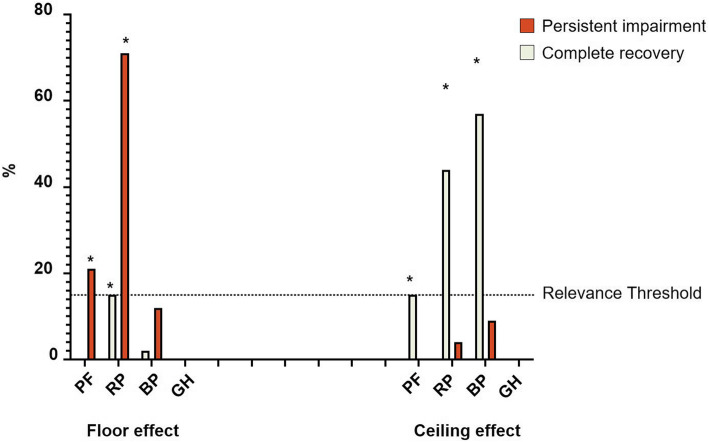
One hundred fifty-nine patients completed 24 months of follow-up, presenting overall low PCS scores. Two distinct sub-cohorts were identified, exhibiting complete recovery or persistent impairment. A third sub-cohort could not be classified into either trajectory. Age, education level and number of co-morbidities were independent determinants of poor recovery (AUROC 0.743 ((95%CI 0.659-0.826), p < 0.001). Those with complete recovery trajectories demonstrated high levels of ceiling effects in physical function (PF) (15%), role physical (RP) (45%) and body pain (BP) (57%) domains of the SF-36. Those with persistent impairment demonstrated high levels of floor effects in the same domains: PF (21%), RP (71%) and BP (12%). The PF domain demonstrated high responsiveness between ICU discharge and at 6 months and was predictive of a persistent impairment trajectory (AUROC 0.859 (95%CI 0.804-0.914), p < 0.001).
Within sepsis survivors, two distinct recovery trajectories of physical recovery were demonstrated. Older patients with more co-morbidities and lower educational achievements were more likely to have a persistent physical impairment trajectory. In regard to trajectory prediction, the PF score of the SF-36 was more responsive than the PCS and could be considered for primary outcomes. Future trials should consider adaptive trial designs that can deal with non-responders or sub-cohort specific outcome measures more effectively.
从重症中存活下来的患者会遭受严重的身体残疾。康复策略对健康相关生活质量的影响并不一致,人群异质性被认为是一个潜在的混杂因素。本二次分析旨在:(1) 研究重症患者的功能恢复轨迹,以描绘亚表型;(2) 评估这些队列在临床特征和身体功能评估工具的计量特性方面的差异。
通过电话访谈对 291 例成年脓毒症幸存者进行了 24 个月的随访。使用 Short Form-36 Questionnaire (SF-36) 的生理成分评分 (PCS)、日常生活活动和 Extra Short Musculoskeletal Function Assessment (XSFMA-F/B) 评估生理功能。通过因子分析对纵向轨迹进行聚类。应用逻辑回归分析确定可能决定聚类分配的患者特征。在聚类内评估反应性、地板和天花板效应以及同时效性。
159 例患者完成了 24 个月的随访,总体 PCS 评分较低。确定了两个不同的亚群,表现为完全恢复或持续受损。第三个亚群无法归入任何轨迹。年龄、教育程度和合并症数量是恢复不良的独立决定因素 (AUROC 0.743((95%CI 0.659-0.826),p<0.001)。完全恢复轨迹的患者在 SF-36 的身体功能 (PF) (15%)、身体角色 (RP) (45%)和身体疼痛 (BP) (57%) 领域表现出高水平的天花板效应。持续受损的患者在同一领域表现出高水平的地板效应:PF (21%)、RP (71%)和 BP (12%)。PF 领域在 ICU 出院时和 6 个月时具有较高的反应性,并且可以预测持续受损的轨迹 (AUROC 0.859(95%CI 0.804-0.914),p<0.001)。
在脓毒症幸存者中,展示了两种不同的身体恢复轨迹。年龄较大、合并症较多、教育程度较低的患者更有可能出现持续性身体损伤轨迹。关于轨迹预测,SF-36 的 PF 评分比 PCS 更敏感,可以考虑作为主要结果。未来的试验应考虑适应性试验设计,以便更有效地处理无反应者或亚组特定的结果测量。