Department of Pediatrics, Johns Hopkins University School of Medicine, 200 N Wolfe St., Room 3055, Baltimore, MD, 21287, USA.
Department of Surgery, Johns Hopkins University School of Medicine, Baltimore, MD, USA.
Pediatr Nephrol. 2021 Jan;36(1):143-151. doi: 10.1007/s00467-020-04764-4. Epub 2020 Sep 26.
In March 2020, COVID-19 infections began to rise exponentially in the USA, placing substantial burden on the healthcare system. As a result, there was a rapid change in transplant practices and policies, with cessation of most procedures. Our goal was to understand changes to pediatric kidney transplantation (KT) at the national level during the COVID-19 epidemic.
Using SRTR data, we examined changes in pediatric waitlist registration, waitlist removal or inactivation, and deceased donor and living donor (DDKT/LDKT) events during the start of the disease transmission in the USA compared with the same time the previous year.
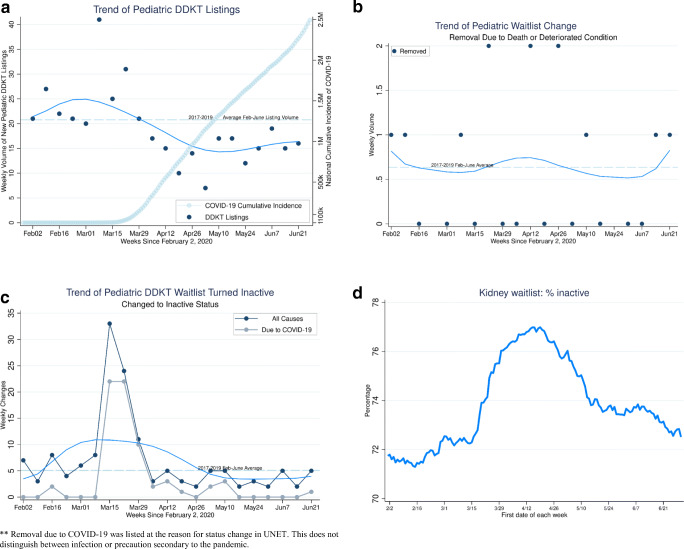
We saw an initial decrease in DDKT and LDKT by 47% and 82% compared with expected events and then a continual increase, with numbers reaching expected prepandemic levels by May 2020. In the early phase of the pandemic, waitlist inactivation and removals due to death or deteriorating condition rose above expected values by 152% and 189%, respectively. There was a statistically significant decrease in new waitlist additions (IRR 0.65 ) and LDKT (IRR 0.38 ) in states with high vs. low COVID activity. Transplant recipients during the pandemic were more likely to have received a DDKT, but had similar calculated panel-reactive antibody (cPRA) values, waitlist time, and cause of kidney failure as before the pandemic.
The COVID-19 pandemic initially reduced access to kidney transplantation among pediatric patients in the USA but has not had a sustained effect.
2020 年 3 月,美国的 COVID-19 感染开始呈指数级增长,给医疗系统带来了巨大的负担。因此,移植实践和政策迅速发生变化,大多数手术都停止了。我们的目标是了解 COVID-19 疫情期间全国范围内儿科肾脏移植(KT)的变化。
使用 SRTR 数据,我们检查了美国疾病传播开始时与前一年同期相比,儿科候补名单登记、候补名单删除或停用以及已故供体和活体供体(DDKT/LDKT)事件的变化。
与预期事件相比,我们最初看到 DDKT 和 LDKT 分别减少了 47%和 82%,然后持续增加,到 2020 年 5 月,数量达到了大流行前的预期水平。在大流行的早期阶段,由于死亡或病情恶化而导致的候补名单停用和删除分别比预期值高出 152%和 189%。与 COVID 活动低的州相比,高 COVID 活动州的新候补名单增加(IRR 0.65)和 LDKT(IRR 0.38)数量均呈统计学显著下降。大流行期间接受移植的患者更有可能接受 DDKT,但与大流行前相比,他们的计算面板反应性抗体(cPRA)值、候补名单时间和肾衰竭原因相似。
COVID-19 大流行最初减少了美国儿科患者获得肾脏移植的机会,但没有持续的影响。