Department of Neurosurgery, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences; Graduate School of Peking Union Medical College, Beijing, 100730, People's Republic of China.
Department of Neurosurgery, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing, 100730, People's Republic of China.
Clin Interv Aging. 2020 Sep 8;15:1611-1624. doi: 10.2147/CIA.S257931. eCollection 2020.
This study aimed to identify independent predictors for the risk of hemorrhagic transformation (HT) in arterial ischemic stroke (AIS) patients.
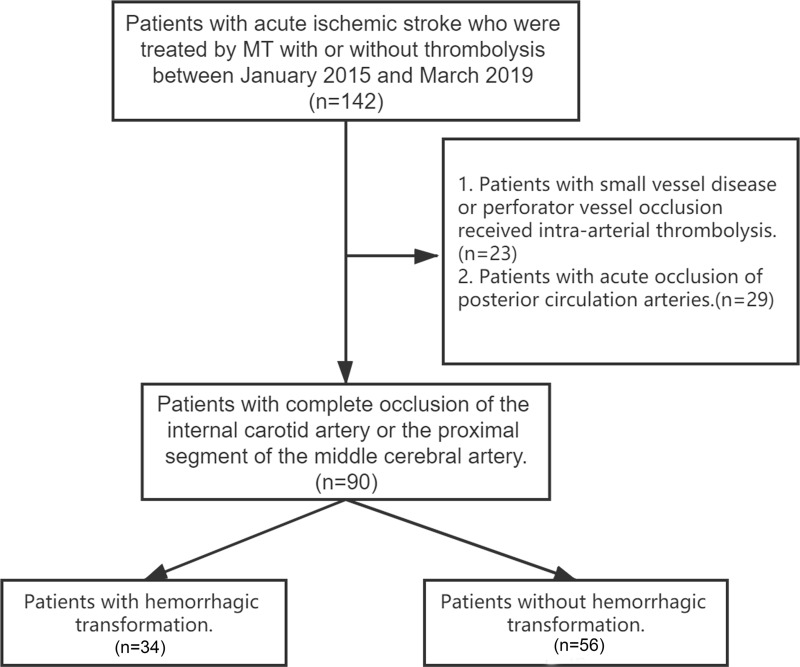
Consecutive patients with AIS due to large artery occlusion in the anterior circulation treated with mechanical thrombectomy (MT) were enrolled in a tertiary stroke center. Demographic and medical history data, admission lab results, and Circle of Willis (CoW) variations were collected from all patients.
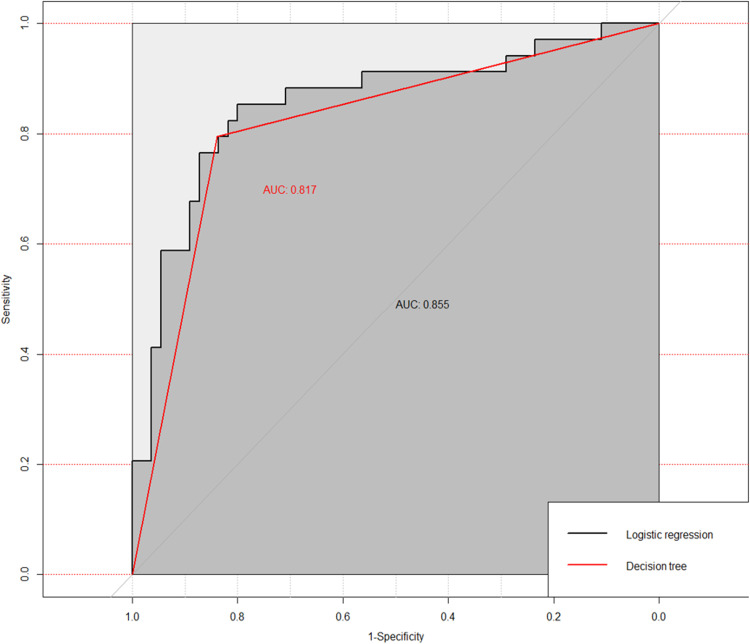
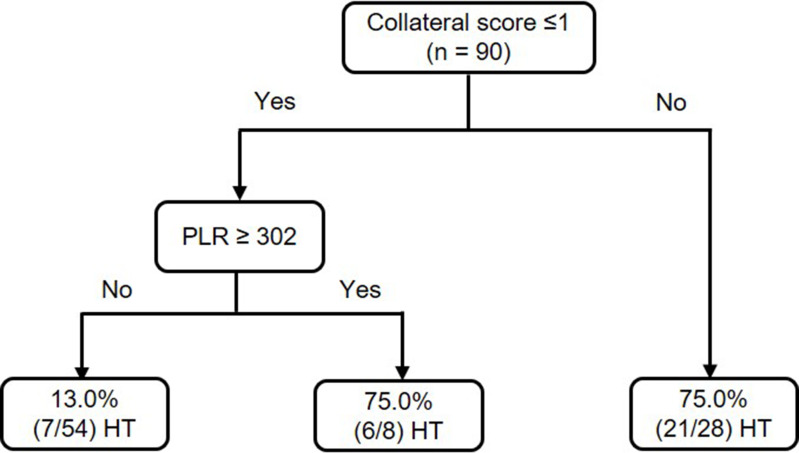
Altogether, 90 patients were included in this study; among them, 34 (37.8%) had HT after MT. The final pruned decision tree (DT) model consisted of collateral score and platelet to lymphocyte ratios (PLR) as predictors. Confusion matrix analysis showed that 82.2% (74/90) were correctly classified by the model (sensitivity, 79.4%; specificity, 83.9%). The area under the ROC curve (AUC) was 81.7%. The DT model demonstrated that participants with collateral scores of 2-4 had a 75.0% probability of HT. For participants with collateral scores of 0-1, if PLR at admission was <302, participants had a 13.0% probability of HT; otherwise, participants had an 75.0% probability of HT. The final adjusted multivariate logistic regression analysis indicated that collateral score 0-1 (OR, 10.186; 95% CI, 3.029-34.248; p < 0.001), PLR (OR, 1.005; 95% CI, 1.001-1.010; p = 0.040), and NIHSS at admission (OR, 1.106; 95% CI, 1.014-1.205; p = 0.022) could be used to predict HT. The AUC for the model was 0.855, with 83.3% (75/90) were correctly classified (sensitivity, 79.4%; specificity, 87.3%). Less patients with HT achieved independent outcomes (mRS, 0-2) in 90 days (20.6% vs. 64.3%, p < 0.001). Rate of poor outcomes (mRS, 4-6) was significantly higher in patients with HT (73.5% vs. 19.6%; p < 0.001).
Both the DT model and multivariate logistic regression model confirmed that the lower collateral status and the higher PLR were significantly associated with an increased risk for HT in AIS patients after MT. PLR may be one of the cost-effective and practical predictors for HT. Further prospective multicenter studies are needed to validate our findings.
本研究旨在确定接受机械血栓切除术(MT)治疗的大动脉闭塞性急性缺血性卒中(AIS)患者发生出血性转化(HT)的独立预测因素。
连续纳入在三级卒中中心接受 MT 治疗的前循环大动脉闭塞性 AIS 患者。收集所有患者的人口统计学和病史数据、入院实验室结果以及 Willis 环(CoW)变异情况。
本研究共纳入 90 例患者,其中 34 例(37.8%)在 MT 后发生 HT。最终修剪后的决策树(DT)模型由侧支评分和血小板与淋巴细胞比值(PLR)作为预测因子组成。混淆矩阵分析显示,模型正确分类了 82.2%(74/90)的患者(敏感性为 79.4%,特异性为 83.9%)。ROC 曲线下面积(AUC)为 81.7%。DT 模型显示,侧支评分为 2-4 分的患者发生 HT 的概率为 75.0%。对于侧支评分为 0-1 分的患者,如果入院时的 PLR<302,则发生 HT 的概率为 13.0%;否则,发生 HT 的概率为 75.0%。最终的多变量调整逻辑回归分析表明,侧支评分 0-1(OR,10.186;95%CI,3.029-34.248;p<0.001)、PLR(OR,1.005;95%CI,1.001-1.010;p=0.040)和入院时 NIHSS(OR,1.106;95%CI,1.014-1.205;p=0.022)可用于预测 HT。模型的 AUC 为 0.855,83.3%(75/90)的患者被正确分类(敏感性为 79.4%,特异性为 87.3%)。在 90 天内,发生 HT 的患者独立结局(mRS,0-2)的比例较低(20.6%比 64.3%,p<0.001)。发生 HT 的患者预后不良(mRS,4-6)的比例显著更高(73.5%比 19.6%;p<0.001)。
DT 模型和多变量逻辑回归模型均证实,较低的侧支状态和较高的 PLR 与 MT 后 AIS 患者 HT 的风险增加显著相关。PLR 可能是 HT 的一种具有成本效益和实用的预测因子。需要进一步的前瞻性多中心研究来验证我们的研究结果。