Child Health and Development Center, Makerere University College of Health Sciences, Kampala, Uganda.
Department of Pediatrics, Division of Nephrology, Indiana University School of Medicine, Indianapolis, Indiana, USA.
BMC Nephrol. 2020 Sep 29;21(1):417. doi: 10.1186/s12882-020-02076-1.
Acute kidney injury (AKI) is increasingly recognized as a consequential clinical complication in children with severe malaria. However, approaches to estimate baseline creatinine (bSCr) are not standardized in this unique patient population. Prior to wide-spread utilization, bSCr estimation methods need to be evaluated in many populations, particularly in children from low-income countries.
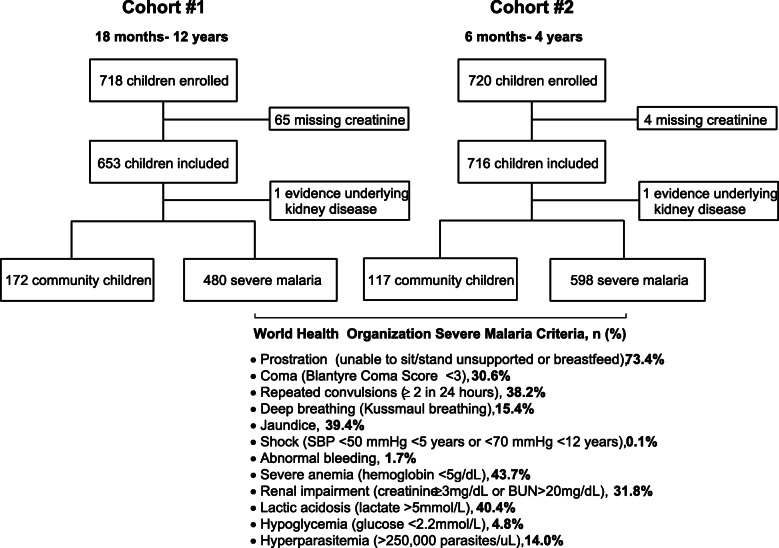
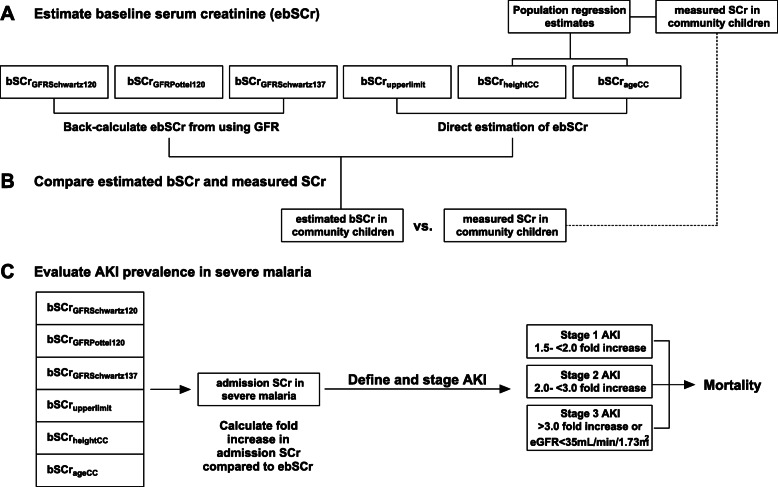
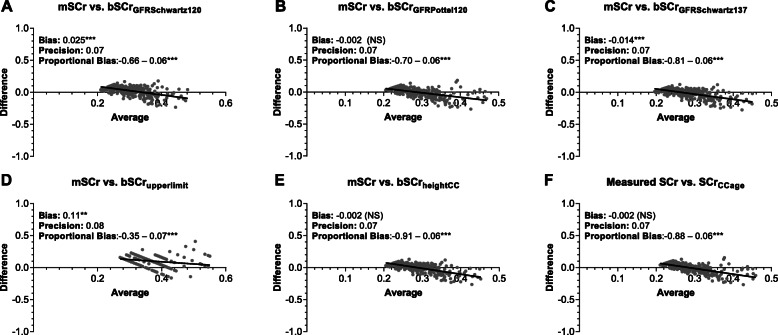
We evaluated six methods to estimate bSCr in Ugandan children aged 6 months to 12 years of age in two cohorts of children with severe malaria (n = 1078) and healthy community children (n = 289). Using isotope dilution mass spectrometry (IDMS)-traceable creatinine measures from community children, we evaluated the bias, accuracy and precision of estimating bSCr using height-dependent and height-independent estimated glomerular filtration (eGFR) equations to back-calculate bSCr or estimating bSCr directly using published or population-specific norms.
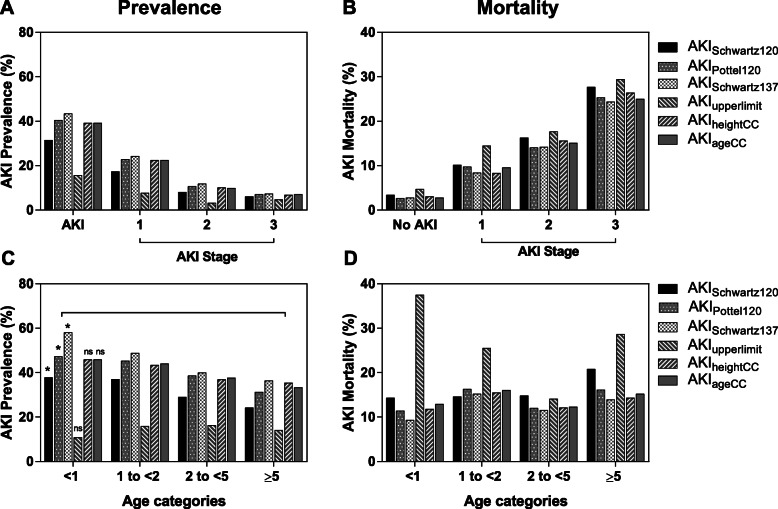
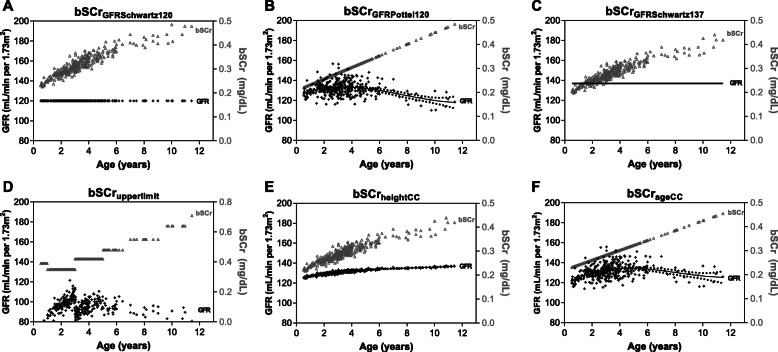
We compared methods to estimate bSCr in healthy community children against the IDMS-traceable SCr measure. The Pottel-age based equation, assuming a normal GFR of 120 mL/min per 1.73m, was the more accurate method with minimal bias when compared to the Schwartz height-based equation. Using the different bSCr estimates, we demonstrated the prevalence of KDIGO-defined AKI in children with severe malaria ranged from 15.6-43.4%. The lowest estimate was derived using population upper levels of normal and the highest estimate was derived using the mean GFR of the community children (137 mL/min per 1.73m) to back-calculate the bSCr. Irrespective of approach, AKI was strongly associated with mortality with a step-wise increase in mortality across AKI stages (p < 0.0001 for all). AKI defined using the Pottel-age based equation to estimate bSCr showed the strongest relationship with mortality with a risk ratio of 5.13 (95% CI 3.03-8.68) adjusting for child age and sex.
We recommend using height-independent age-based approaches to estimate bSCr in hospitalized children in sub-Saharan Africa due to challenges in accurate height measurements and undernutrition which may impact bSCr estimates. In this population the Pottel-age based GFR estimating equation obtained comparable bSCr estimates to population-based estimates in healthy children.
急性肾损伤(AKI)在重症疟疾患儿中日益被认为是一种严重的临床并发症。然而,在这个特殊的患者群体中,估计基础肌酐(bSCr)的方法尚未标准化。在广泛应用之前,需要在许多人群中评估 bSCr 估计方法,特别是在来自低收入国家的儿童中。
我们评估了六种方法,用于估计乌干达 6 个月至 12 岁患有严重疟疾的儿童(n=1078)和健康社区儿童(n=289)的 bSCr。使用来自社区儿童的同位素稀释质谱法(IDMS)可追踪肌酐测量值,我们评估了使用依赖身高和不依赖身高的估计肾小球滤过率(eGFR)方程回溯计算 bSCr 或直接使用已发表或人群特异性标准估计 bSCr 的方法的偏倚、准确性和精密度。
我们将健康社区儿童的 bSCr 估计方法与 IDMS 可追踪的 SCr 测量值进行了比较。基于 Pottel 年龄的方程,假设 GFR 正常为 120mL/min/1.73m,与 Schwartz 基于身高的方程相比,具有最小的偏差,是更准确的方法。使用不同的 bSCr 估计值,我们表明严重疟疾患儿中 KDIGO 定义的 AKI 的患病率范围为 15.6-43.4%。最低估计值是使用人群正常上限值计算得出的,而最高估计值是使用社区儿童的平均 GFR(137mL/min/1.73m)回溯计算得出的 bSCr。无论采用哪种方法,AKI 均与死亡率密切相关,随着 AKI 阶段的逐步增加,死亡率呈阶梯式上升(p<0.0001 均)。使用基于 Pottel 年龄的方程估计 bSCr 定义的 AKI 与死亡率的关系最强,在校正儿童年龄和性别后,风险比为 5.13(95%CI 3.03-8.68)。
我们建议在撒哈拉以南非洲的住院儿童中使用不依赖身高的基于年龄的方法来估计 bSCr,因为身高测量和营养不良的准确性可能会影响 bSCr 估计。在该人群中,基于 Pottel 年龄的 GFR 估计方程与健康儿童的基于人群的估计值获得了可比的 bSCr 估计值。