Department of Neurosurgery, Charité Universitätsmedizin Berlin, corporate member of Freie Universität Berlin, Humboldt-Universität zu Berlin, and Berlin Institute of Health, Charitéplatz 1, 10117, Berlin, Germany.
Berlin Institute of Health (BIH), Anna-Louisa-Karsch-Str. 2, 10178, Berlin, Germany.
Radiat Oncol. 2020 Sep 29;15(1):225. doi: 10.1186/s13014-020-01655-8.
Stereotactic radiosurgery (SRS) has been increasingly applied for up to 10 brain metastases instead of whole brain radiation therapy (WBRT) to achieve local tumor control while reducing neurotoxicity. Furthermore, brain-metastasis incidence is rising due to the increasing survival of patients with cancer. Our aim was to analyze the efficacy and safety of CyberKnife (CK) radiosurgery for elderly patients.
We retrospectively identified all patients with brain metastases ≥ 65 years old treated with CK-SRS at our institution since 2011 and analyzed data of primary diseases, multimodality treatments, and local therapy effect based on imaging follow-up and treatment safety. Kaplan-Meier analysis for local progression-free interval and overall survival were performed.
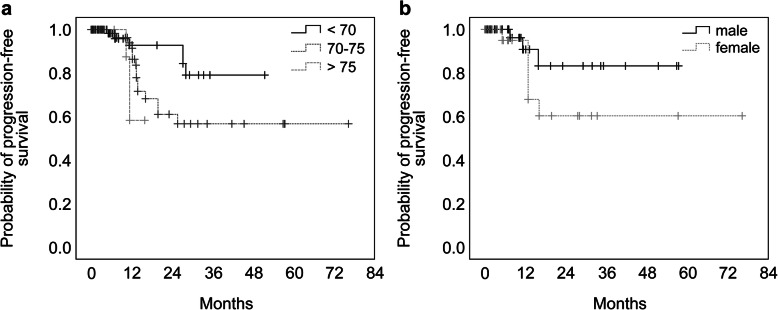
We identified 97 patients (233 lesions) fulfilling the criteria at the first CK-SRS. The mean age was 73.2 ± 5.8 (range: 65.0-87.0) years. Overall, 13.4% of the patients were > 80 years old. The three most frequent primary cancers were lung (40.2%), kidney (22.7%), and malignant melanoma (15.5%). In 38.5% (47/122 treatments) multiple brain metastases were treated with the CK-SRS, with up to eight lesions in one session. The median planning target volume (PTV) was 1.05 (range: 0.01-19.80) cm. A single fraction was applied in 92.3% of the lesions with a median prescription dose of 19 (range: 12-21) Gy. The estimated overall survivals at 3-, 6-, and 12 months after SRS were 79, 55, and 23%, respectively. The estimated local tumor progression-free intervals at 6-, 12-, 24-, 36-, and 72 months after SRS were 99.2, 89.0, 67.2, 64.6, and 64.6%, respectively. Older age and female sex were predictive factors of local progression. The Karnofsky performance score remained stable in 97.9% of the patients; only one patient developed a neurological deficit after SRS of a cerebellar lesion (ataxia, CTCAE Grade 2).
SRS is a safe and efficient option for the treatment of elderly patients with brain metastases with good local control rates without the side effects of WBRT. Older age and female sex seem to be predictive factors of local progression. Prospective studies are warranted to clarify the role of SRS treatment for elderly patients.
立体定向放射外科(SRS)已越来越多地用于治疗多达 10 个脑转移瘤,以实现局部肿瘤控制,同时减少神经毒性。此外,由于癌症患者的生存率不断提高,脑转移瘤的发病率也在上升。我们的目的是分析 CyberKnife(CK)放射外科治疗老年患者的疗效和安全性。
我们回顾性地确定了自 2011 年以来在我们机构接受 CK-SRS 治疗的所有年龄≥65 岁的脑转移瘤患者,并根据影像学随访和治疗安全性分析了原发疾病、多模态治疗和局部治疗效果的数据。对局部无进展生存期和总生存期进行 Kaplan-Meier 分析。
我们在第一次 CK-SRS 中确定了 97 名(233 个病灶)符合标准的患者。平均年龄为 73.2±5.8(范围:65.0-87.0)岁。总体而言,13.4%的患者年龄超过 80 岁。最常见的三种原发癌是肺癌(40.2%)、肾癌(22.7%)和恶性黑色素瘤(15.5%)。38.5%(47/122 例治疗)的患者接受了 CK-SRS 治疗多个脑转移瘤,一次治疗多达 8 个病灶。中位计划靶区(PTV)为 1.05(范围:0.01-19.80)cm。92.3%的病变采用单次分割,处方剂量中位数为 19(范围:12-21)Gy。SRS 后 3、6 和 12 个月的总生存率分别为 79%、55%和 23%。SRS 后 6、12、24、36 和 72 个月的局部肿瘤无进展间隔估计分别为 99.2%、89.0%、67.2%、64.6%和 64.6%。年龄较大和女性是局部进展的预测因素。97.9%的患者卡氏行为状态评分保持稳定;仅有 1 例患者在小脑病变 SRS 后出现神经功能缺损(共济失调,CTCAE 分级 2)。
SRS 是治疗老年脑转移瘤的一种安全有效的方法,具有良好的局部控制率,无 WBRT 的副作用。年龄较大和女性似乎是局部进展的预测因素。需要前瞻性研究来阐明 SRS 治疗老年患者的作用。