Jongeneel Gabrielle, Greuter Marjolein J E, van Erning Felice N, Koopman Miriam, Vink Geraldine R, Punt Cornelis J A, Coupé Veerle M H
Department of Epidemiology and Biostatistics, Amsterdam UMC, VU University, PO Box 7057, MF F-wing, Amsterdam, 1007 MB, The Netherlands.
Department of Epidemiology and Biostatistics, VU University, Amsterdam, The Netherlands.
Therap Adv Gastroenterol. 2020 Sep 16;13:1756284820954114. doi: 10.1177/1756284820954114. eCollection 2020.
Our aim was to evaluate the cost effectiveness of 3 months' adjuvant chemotherapy 6 months in high-risk (T4 stage + microsatellite stable) stage II colon cancer (CC) patients.
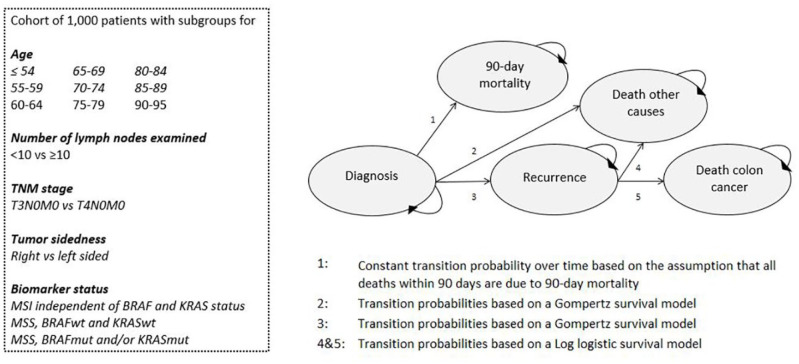
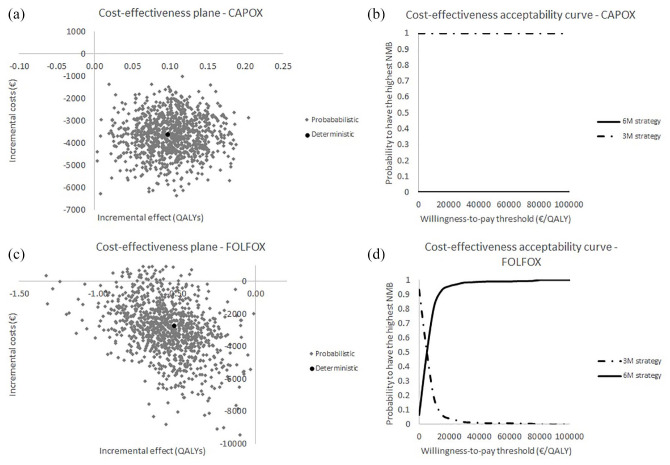
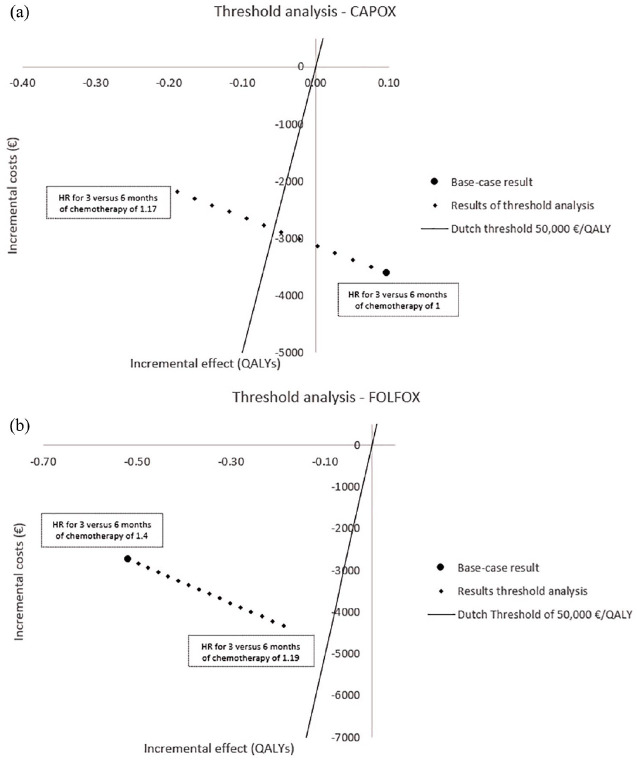
Using the validated PATTERN Markov cohort model, which simulates the disease progression of stage II CC patients from diagnosis to death, we first evaluated a reference strategy in which high-risk patients were treated with chemotherapy for 6 months. In the second strategy, treatment duration was shortened to 3 months. Both strategies were evaluated for CAPOX (capecitabine plus oxaliplatin) and FOLFOX (fluorouracil, leucovorin and oxaliplatin). Based on trial data, we assumed that shortened treatment duration compared with a 6-month regimen was equally effective for CAPOX and less effective for FOLFOX. Adverse events were highest in the 6-month strategy. Analyses were conducted from a societal perspective using a lifelong time horizon. Outcomes were number of CC deaths per 1000 patients and total discounted costs and quality-adjusted life-years (QALYs) per patient (pp). Incremental net monetary benefit (iNMB) was calculated using a willingness-to-pay value of €50,000/QALY.
For CAPOX, the 6-month strategy resulted in 316 CC deaths per 1000 patients, 6.71 QALYs pp and total costs of €41,257 pp. The 3-month strategy resulted in an equal number of CC deaths, but higher QALYs (6.80 pp) and lower costs (€37,645 pp), leading to a iNMB of €8454 per person for 3 months 6 months. For FOLFOX, the 6-month strategy resulted in 316 CC deaths per 1000 patients, 6.71 QALYs pp and total costs of €47,135 pp. The 3-month strategy resulted in more CC deaths (393), lower QALYs (6.19 pp) and lower costs (€44,389 pp). An iNMB of -€23,189 was found for 3 months 6 months.
Our findings indicate that 3 months' adjuvant chemotherapy should be considered as standard of care in high-risk stage II CC patients for CAPOX, but not for FOLFOX.
我们的目的是评估高危(T4期+微卫星稳定)II期结肠癌(CC)患者接受3个月辅助化疗而非6个月辅助化疗的成本效益。
使用经过验证的PATTERN马尔可夫队列模型,该模型模拟II期CC患者从诊断到死亡的疾病进展,我们首先评估了一种参考策略,即高危患者接受6个月的化疗。在第二种策略中,治疗时间缩短至3个月。两种策略都针对CAPOX(卡培他滨加奥沙利铂)和FOLFOX(氟尿嘧啶、亚叶酸钙和奥沙利铂)进行了评估。根据试验数据,我们假设与6个月疗程相比,缩短治疗时间对CAPOX同样有效,而对FOLFOX效果较差。6个月策略中的不良事件发生率最高。从社会角度使用终身时间范围进行分析。结果是每1000名患者的CC死亡人数以及每名患者(pp)的总贴现成本和质量调整生命年(QALY)。使用50000欧元/QALY的支付意愿值计算增量净货币效益(iNMB)。
对于CAPOX,6个月策略导致每1000名患者中有316例CC死亡,每名患者6.71个QALY,总费用为每名患者41257欧元。3个月策略导致的CC死亡人数相同,但QALY更高(6.80 pp),成本更低(37645欧元/pp),3个月而非6个月的iNMB为每人8454欧元。对于FOLFOX,6个月策略导致每1000名患者中有316例CC死亡,每名患者6.71个QALY,总费用为每名患者47135欧元。3个月策略导致更多CC死亡(393例),QALY更低(6.19 pp),成本更低(44389欧元/pp)。3个月而非6个月的iNMB为-23189欧元。
我们的研究结果表明,对于CAPOX,3个月辅助化疗应被视为高危II期CC患者的标准治疗方案,但对于FOLFOX则不然。