Brown Janet E, Handforth Catherine, Compston Juliet E, Cross William, Parr Nigel, Selby Peter, Wood Steven, Drudge-Coates Lawrence, Walsh Jennifer S, Mitchell Caroline, Collinson Fiona J, Coleman Robert E, James Nicholas, Francis Roger, Reid David M, McCloskey Eugene
Academic Unit of Clinical Oncology, Department of Oncology and Metabolism, University of Sheffield, United Kingdom.
Department of Medicine, Cambridge Biomedical Campus, United Kingdom.
J Bone Oncol. 2020 Aug 2;25:100311. doi: 10.1016/j.jbo.2020.100311. eCollection 2020 Dec.
Incidence of prostate cancer (PC) is increasing, but androgen deprivation therapy (ADT) and other therapies are substantially improving survival. In this context, careful consideration of skeletal health is required to reduce the risk of treatment-related fragility fractures and their associated morbidity and mortality. This risk is currently not well-managed. ADT causes significant loss of bone mineral density (BMD). In the metastatic setting, systemic treatments (e.g. chemotherapy, abiraterone, enzalutamide) are used alongside ADT and may require concomitant glucocorticoids. Both ADT and glucocorticoids pose significant challenges to skeletal health in a population of patients already likely to have ongoing age-related bone loss and/or comorbid conditions. Current PC guidelines lack specific recommendations for optimising bone health. This guidance presents evidence for assessment and management of bone health in this population, with specific recommendations for clinical practitioners in day-to-day PC management.
Structured meetings of key opinion leaders were integrated with a systematic literature review. Input and endorsement was sought from patients, nursing representatives and specialist societies.
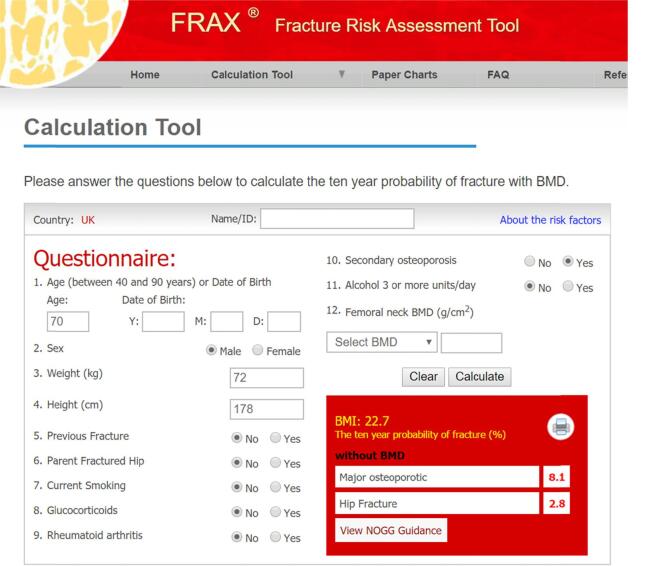
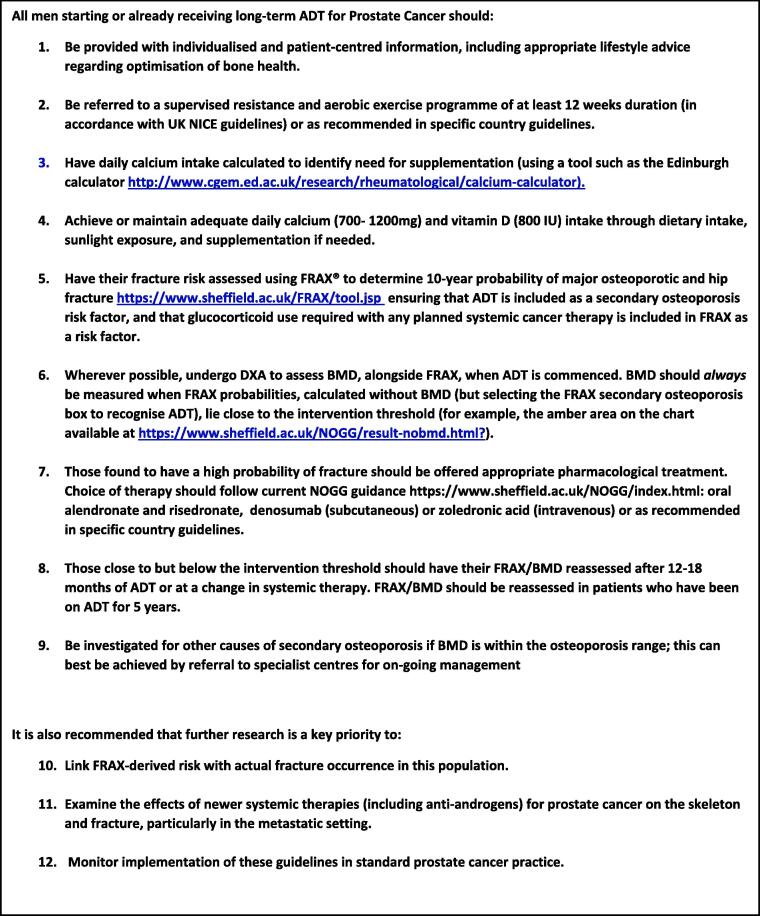
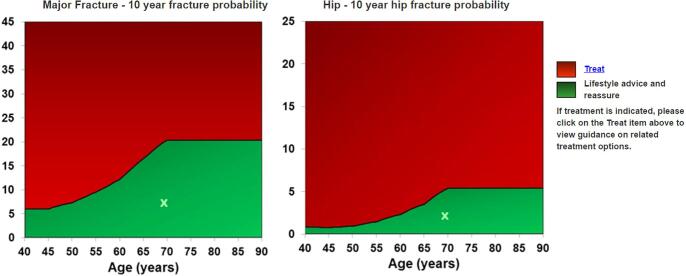
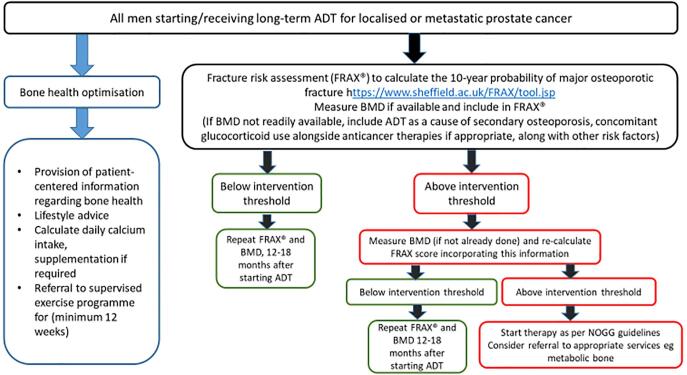
All men starting or continuing long-term ADT should receive lifestyle advice regarding bone health. Calcium/vitamin D supplementation should be offered if required. Fracture risk should be calculated (using the FRAX® tool), with BMD assessment included where feasible. BMD should always be assessed where fracture risk calculated using FRAX® alone is close to the intervention threshold. Intervention should be provided if indicated by local or national guidelines e.g. UK National Osteoporosis Guideline Group (NOGG) thresholds. Men requiring bone protection therapy should be further assessed (e.g. renal function), with referral to specialist centres if available and offered appropriate treatment to reduce fracture risk. Those near to, but below an intervention threshold, and patients going on to additional systemic therapies (particularly those requiring glucocorticoids), should have FRAX® (including BMD) repeated after 12-18 months.
Modern treatments for prostate cancer have led to significant improvements in survival and quality of life. However, some of these treatments may lead to weakening of patient's bones with risk of fracture and it is therefore important to monitor patients' bone health and provide bone protection where needed. This paper provides specific guidance to clinical teams, based on the most recent research evidence, to ensure optimal bone health in their patients.
前列腺癌(PC)的发病率正在上升,但雄激素剥夺疗法(ADT)和其他疗法正在显著提高生存率。在此背景下,需要仔细考虑骨骼健康,以降低与治疗相关的脆性骨折风险及其相关的发病率和死亡率。目前这种风险管理不善。ADT会导致骨矿物质密度(BMD)显著降低。在转移性情况下,全身治疗(如化疗、阿比特龙、恩杂鲁胺)与ADT联合使用,可能需要同时使用糖皮质激素。ADT和糖皮质激素对本就可能存在与年龄相关的持续骨质流失和/或合并症的患者群体的骨骼健康都构成了重大挑战。当前的PC指南缺乏优化骨骼健康的具体建议。本指南提供了该人群骨骼健康评估和管理的证据,并为PC日常管理中的临床医生提供了具体建议。
关键意见领袖的结构化会议与系统的文献综述相结合。征求了患者、护理代表和专业协会的意见并获得认可。
所有开始或继续长期ADT治疗的男性都应接受有关骨骼健康的生活方式建议。如有需要,应提供钙/维生素D补充剂。应计算骨折风险(使用FRAX®工具),并在可行的情况下进行BMD评估。如果仅使用FRAX®计算出的骨折风险接近干预阈值,则应始终评估BMD。如果当地或国家指南(如英国国家骨质疏松症指南小组(NOGG)阈值)表明需要干预,则应进行干预。需要骨保护治疗的男性应进一步评估(如肾功能),如有可能应转诊至专科中心,并提供适当治疗以降低骨折风险。那些接近但低于干预阈值的患者,以及继续接受其他全身治疗(特别是那些需要糖皮质激素的患者),应在12 - 18个月后重复进行FRAX®(包括BMD)评估。
现代前列腺癌治疗方法已使生存率和生活质量有了显著提高。然而,其中一些治疗方法可能会导致患者骨骼变弱,有骨折风险,因此监测患者的骨骼健康并在需要时提供骨骼保护非常重要。本文基于最新研究证据为临床团队提供了具体指导,以确保患者的骨骼健康达到最佳状态。