Department of Urology, Hôpital Foch, Université Paris-Saclay, 40, Rue Worth, 92150, Suresnes, France.
UVSQ-Université Paris-Saclay, Paris, France.
Sci Rep. 2020 Sep 30;10(1):16145. doi: 10.1038/s41598-020-73191-0.
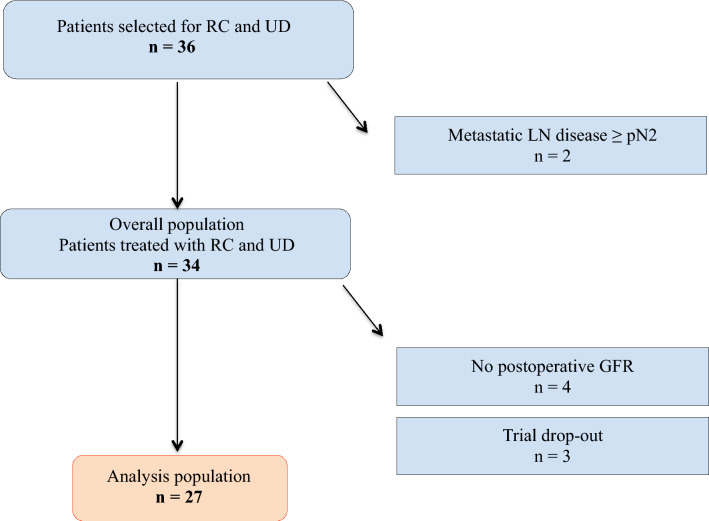
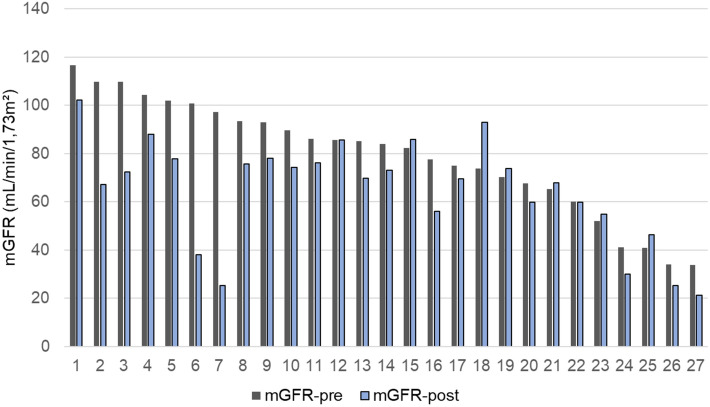
Precise determination of glomerular filtration rate (GFR) is essential for the management of patients with muscle-invasive bladder cancer (MIBC). We aim to describe the early evolution of measured GFR (mGFR) after radical cystectomy and urinary diversion (RCUD) and to identify risk factors for GFR decline. GFR measurement using Cr-EDTA continuous infusion, estimated GFR (eGFR) from five published equations and renal scintigraphy with split renal function determination were performed before and 6 months after RCUD. Chronic Kidney Disease (mGFR < 60 mL/min/1.73 m) and GFR stages were defined according to the KDIGO guidelines using mGFR. Twenty-seven patients (men 85%, median age 65, IQR 59; 68 years) were included. A total of 20 (74%) patients experienced significant mGFR decline at 6 months postoperatively. Median mGFR decreased from 84.1 pre-operatively (IQR 65.3; 97.2) to 69.9 mL/min/1.73 m (IQR 55.0; 77.9) 6 months after surgery (p < 0.001). Thirteen (48%) patients had a progression to a worse GFR stage. Of the 22 patients without pre-operative CKD, 5 (23%) developed post-operative CKD. Diabetes mellitus was more frequent in patients in the highest tertile of relative mGFR decline (44% vs. 11%, p = 0.02) and platinum-based adjuvant chemotherapy tended to be more frequently used in these patients (44% vs. 17%, p = 0.06). Importantly, pre-operative weight was independently and negatively associated with post-operative mGFR and with mGFR slope in multivariable analyses. In this prospective series, we demonstrated that early and significant mGFR decline occurred after RCUD and perioperative platinum-based chemotherapy, especially in patients with diabetes mellitus and overweight.
准确测定肾小球滤过率(GFR)对于肌层浸润性膀胱癌(MIBC)患者的管理至关重要。我们旨在描述根治性膀胱切除术和尿流改道术(RCUD)后测量的 GFR(mGFR)的早期变化,并确定 GFR 下降的危险因素。在 RCUD 之前和之后 6 个月,使用 Cr-EDTA 连续输注测量 GFR,使用五个已发表的方程估计 GFR(eGFR)以及通过肾闪烁照相术测定分肾功能。根据 KDIGO 指南,使用 mGFR 定义慢性肾脏病(mGFR < 60 mL/min/1.73 m)和 GFR 分期。共纳入 27 例患者(85%为男性,中位年龄 65 岁,IQR 59;68 岁)。共有 20 例(74%)患者在术后 6 个月时出现明显的 mGFR 下降。mGFR 中位数从术前的 84.1(IQR 65.3;97.2)下降至术后 6 个月的 69.9 mL/min/1.73 m(IQR 55.0;77.9)(p < 0.001)。13 例(48%)患者的 GFR 分期恶化。在 22 例术前无 CKD 的患者中,有 5 例(23%)术后出现 CKD。在相对 mGFR 下降最高三分位的患者中,糖尿病更为常见(44% vs. 11%,p = 0.02),这些患者更倾向于使用铂类辅助化疗(44% vs. 17%,p = 0.06)。重要的是,在多变量分析中,术前体重与术后 mGFR 以及 mGFR 斜率独立且呈负相关。在本前瞻性系列研究中,我们发现 RCUD 和围手术期铂类化疗后会发生早期和显著的 mGFR 下降,尤其是在患有糖尿病和超重的患者中。