From the Institute of Cognitive and Translational Neuroscience (INCYT), INECO Foundation, Favaloro University, Buenos Aires, Argentina (Abrevaya, Yoris, De la Fuente, Martorell-Caro); National Scientific and Technical Research Council (CONICET), Argentina (Abrevaya, Fittipaldi, García, Birba, Yoris, Salamone, De la Fuente, García-Cordero, Martorell-Caro, Sedeño, Ibáñez); Facultad de Psicología, Universidad Nacional de Córdoba, Córdoba, Argentina (Abrevaya, Fittipaldi, Salamone, Pautassi); Universidad de San Andrés, Buenos Aires, Argentina (Fittipaldi, García, Dottori, Birba, García-Cordero, Martorell-Caro, Ibáñez); Faculty of Education, National University of Cuyo, Mendoza, Argentina (García); Departamento de Lingu[Combining Diaeresis]ística y Literatura, Facultad de Humanidades, Universidad de Santiago de Chile, Santiago, Chile (García); Global Brain Health Institute, University of California, San Francisco, USA (García, Ibáñez); Radiology Hospital Universitario San Ignacio (HUSI), Bogotá, Colombia (Santamaria-Garcia); Chair for Addiction Research, Institute for Clinical Psychology and Psychotherapy, Dresden, Germany (Hildebrandt); Buenos Aires Physics Institute (IFIBA) and Physics Department, University of Buenos Aires, Buenos Aires, Argentina (De la Fuente); Faculty of Human Sciences and Behavior, Favaloro University, Buenos Aires, Argentina (Alarco-Martí); Instituto de Investigación Médica M. y M. Ferreyra, INIMEC-CONICET-UNC, Córdoba, Argentina (Pautassi); Memory and Balance Clinic, Buenos Aires, Argentina (Serrano); Universidad Autónoma del Caribe, Barranquilla, Colombia (Ibáñez); and Department of Psychology, Center for Social and Cognitive Neuroscience, School of Psychology, Universidad Adolfo Ibáñez, Santiago, Chile (Ibáñez).
Psychosom Med. 2020 Nov/Dec;82(9):850-861. doi: 10.1097/PSY.0000000000000868.
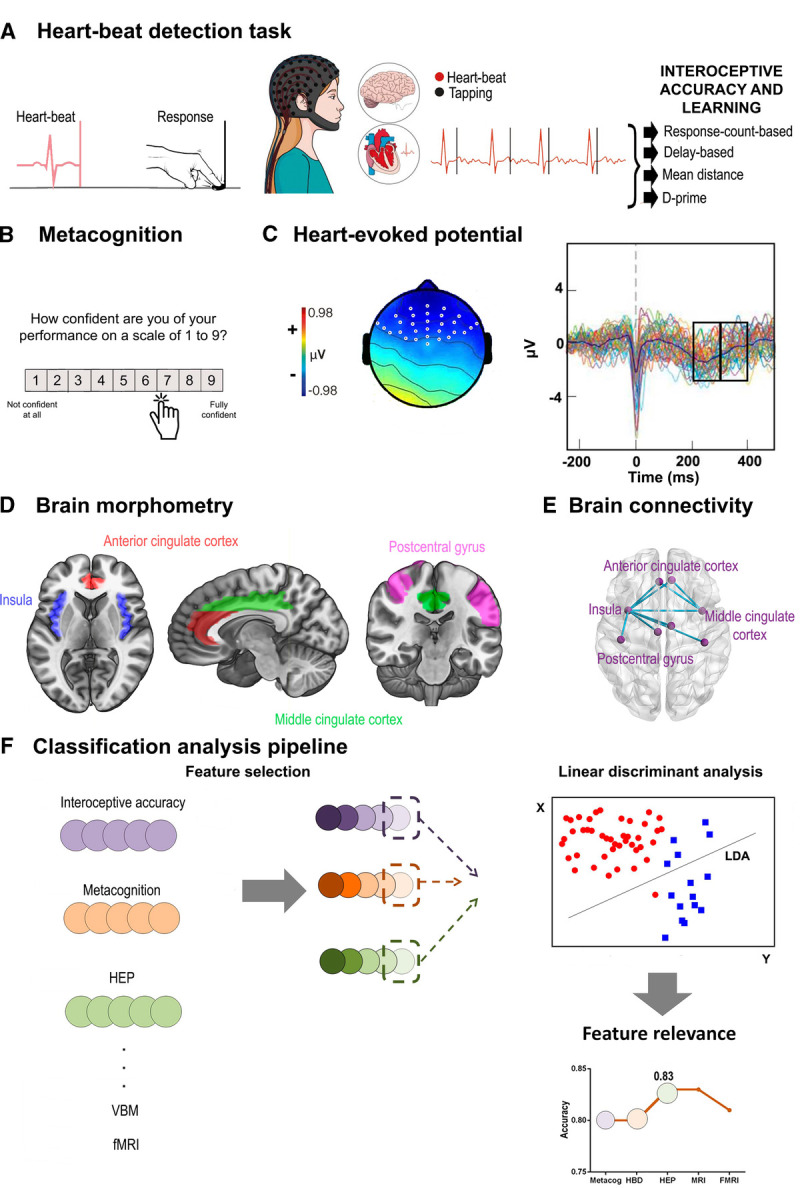
Neurological nosology, based on categorical systems, has largely ignored dimensional aspects of neurocognitive impairments. Transdiagnostic dimensional approaches of interoception (the sensing of visceral signals) may improve the descriptions of cross-pathological symptoms at behavioral, electrophysiological, and anatomical levels. Alterations of cardiac interoception (encompassing multidimensional variables such as accuracy, learning, sensibility, and awareness) and its neural correlates (electrophysiological markers, imaging-based anatomical and functional connectivity) have been proposed as critical across disparate neurological disorders. However, no study has examined the specific impact of neural (relative to autonomic) disturbances of cardiac interoception or their differential manifestations across neurological conditions.
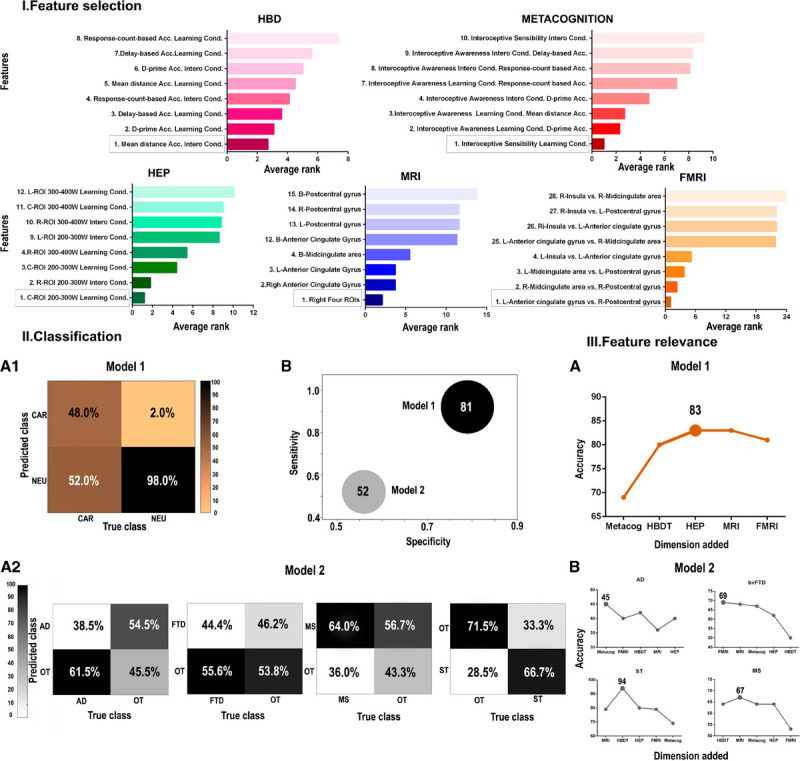
Here, we used a computational approach to classify and evaluate which markers of cardiac interoception (behavioral, metacognitive, electrophysiological, volumetric, or functional) offer the best discrimination between neurological conditions and cardiac (hypertensive) disease (model 1), and among neurological conditions (Alzheimer's disease, frontotemporal dementia, multiple sclerosis, and brain stroke; model 2). In total, the study comprised 52 neurological patients (mean [standard deviation] age = 55.1 [17.3] years; 37 women), 25 cardiac patients (age = 66.2 [9.1] years; 13 women), and 72 healthy controls (age = 52.65 [17.1] years; 50 women).
Cardiac interoceptive outcomes successfully classified between neurological and cardiac conditions (model 1: >80% accuracy) but not among neurological conditions (model 2: 53% accuracy). Behavioral cardiac interoceptive alterations, although present in all conditions, were powerful in differentiating between neurological and cardiac diseases. However, among neurological conditions, cardiac interoceptive deficits presented more undifferentiated and unspecific disturbances across dimensions.
Our result suggests a diffuse pattern of interoceptive alterations across neurological conditions, highlighting their potential role as dimensional, transdiagnostic markers.
基于分类系统的神经疾病分类学在很大程度上忽略了神经认知障碍的维度方面。内脏感觉(感知内脏信号)的跨诊断维度方法可以改善行为、电生理和解剖学水平上跨病理症状的描述。心脏内感受(包括准确性、学习、敏感性和意识等多维变量)及其神经相关性(电生理标志物、基于成像的解剖和功能连接)的改变已被提出是各种神经障碍的关键。然而,尚无研究检查心脏内感受的神经(相对于自主)干扰的特定影响及其在不同神经病症中的差异表现。
在这里,我们使用计算方法来分类和评估心脏内感受的哪些标志物(行为、元认知、电生理、体积或功能)可以在神经病症和心脏(高血压)疾病(模型 1)之间以及在神经病症(阿尔茨海默病、额颞叶痴呆、多发性硬化症和脑卒中等)之间提供最佳区分(模型 2)。总共有 52 名神经科患者(平均[标准差]年龄=55.1[17.3]岁;37 名女性),25 名心脏患者(年龄=66.2[9.1]岁;13 名女性)和 72 名健康对照组(年龄=52.65[17.1]岁;50 名女性)。
心脏内感受结果成功地将神经病症和心脏病症进行分类(模型 1:>80%的准确率),但不能在神经病症之间进行分类(模型 2:53%的准确率)。尽管所有病症中都存在心脏内感受的改变,但行为心脏内感受的改变在区分神经病症和心脏疾病方面非常有力。然而,在神经病症中,心脏内感受缺陷在各个维度上呈现出更加不分化和非特异性的紊乱。
我们的结果表明,跨神经病症存在弥散性的内感受改变,突出了它们作为维度、跨诊断标记物的潜在作用。