Department of Health Service Research and Policy, London School of Hygiene and Tropical Medicine, 15-17 Tavistock Place, London WC1H 9SH, UK
Royal College of Obstetricians and Gynaecologists, London, UK.
BMJ. 2020 Oct 1;371:m3377. doi: 10.1136/bmj.m3377.
To determine the rate of complicated birth at term in women classified at low risk according to the National Institute for Health and Care Excellence guideline for intrapartum care (no pre-existing medical conditions, important obstetric history, or complications during pregnancy) and to assess if the risk classification can be improved by considering parity and the number of risk factors.
Cohort study using linked electronic maternity records.
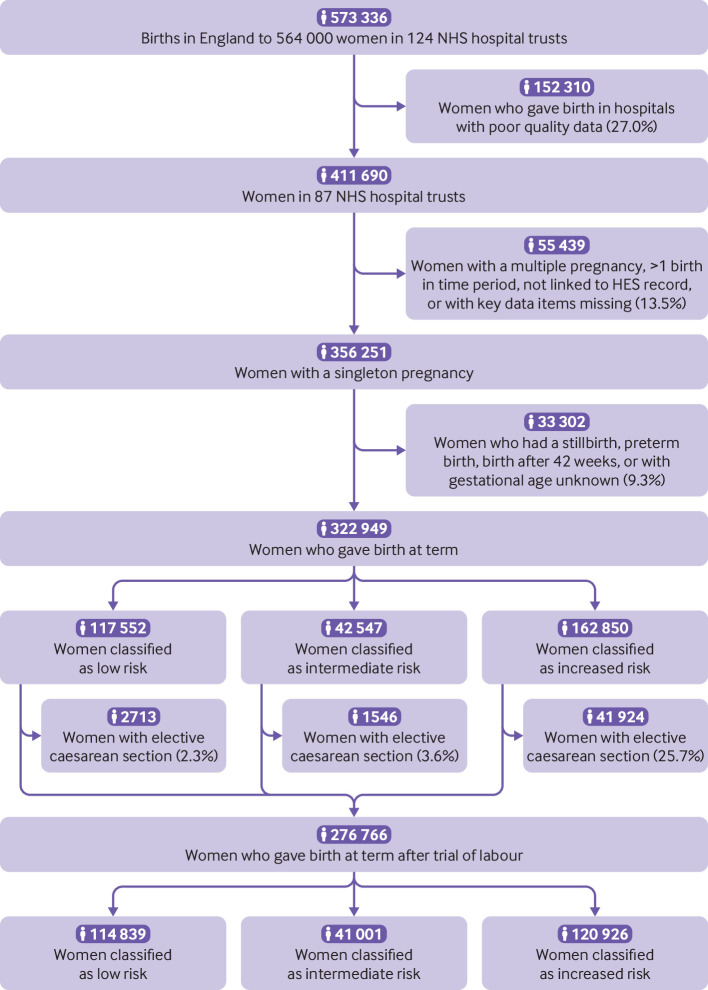
276 766 women with a singleton birth at term after a trial of labour in 87 NHS hospital trusts in England between April 2015 and March 2016.
A composite outcome of complicated birth, defined as a birth with use of an instrument, caesarean delivery, anal sphincter injury, postpartum haemorrhage, or Apgar score of 7 or less at five minutes.
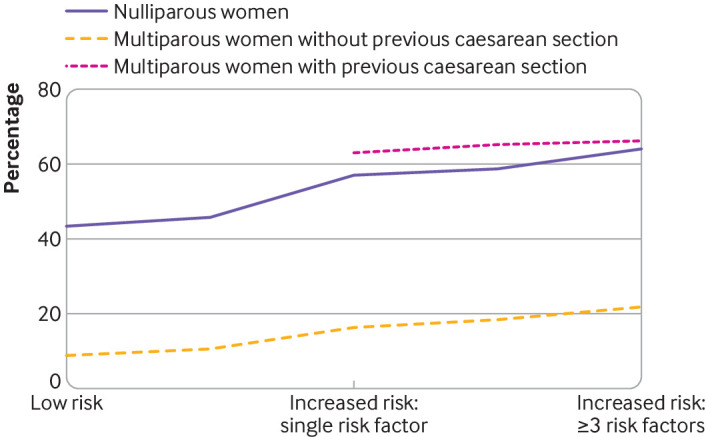
Multiparous women without a history of caesarean section had the lowest rates of complicated birth, varying from 8.8% (4879 of 55 426 women, 95% confidence interval 8.6% to 9.0%) in those without specific risk factors to 21.8% (613 of 2811 women, 20.2% to 23.4%) in those with three or more. The rate of complicated birth was higher in nulliparous women, with corresponding rates varying from 43.4% (25 805 of 59 413 women, 43.0% to 43.8%) to 64.3% (364 of 566 women, 60.3% to 68.3%); and highest in multiparous women with previous caesarean section, with corresponding rates varying from 42.9% (3426 of 7993 women, 41.8% to 44.0%) to 66.3% (554 of 836 women, 63.0% to 69.5%).
Nulliparous women without risk factors have substantially higher rates of complicated birth than multiparous women without a previous caesarean section even if the latter have multiple risk factors. Grouping women first according to parity and previous mode of birth, and then within these groups according to presence of specific risk factors would provide greater and more informed choice to women, better targeting of interventions, and fewer transfers during labour than according to the presence of risk factors alone.
根据英国国家卫生与保健卓越研究所(NICE)分娩期护理指南,确定无既往医学疾病、重要产科病史或妊娠期间无并发症的低危产妇足月分娩时出现复杂分娩的比率,并评估通过考虑生育次数和危险因素数量是否可以改善风险分类。
使用链接电子产妇记录的队列研究。
2015 年 4 月至 2016 年 3 月期间,英格兰 87 家 NHS 医院中有 276766 名经试产后足月单胎分娩的妇女。
复合分娩结局,定义为使用器械分娩、剖宫产、肛门括约肌损伤、产后出血或 5 分钟时 Apgar 评分为 7 分或更低。
无剖宫产史的多产妇分娩复杂的发生率最低,无特定危险因素的产妇发生率为 8.8%(4879/55426 例,95%置信区间 8.6%至 9.0%),而有 3 个或更多危险因素的产妇发生率为 21.8%(613/2811 例,20.2%至 23.4%)。初产妇的分娩复杂发生率更高,相应的发生率从 43.4%(25805/59413 例,43.0%至 43.8%)到 64.3%(364/566 例,60.3%至 68.3%)不等;而有剖宫产史的多产妇发生率最高,相应的发生率从 42.9%(3426/7993 例,41.8%至 44.0%)到 66.3%(554/836 例,63.0%至 69.5%)不等。
即使多产妇无既往剖宫产史且具有多个危险因素,无危险因素的初产妇分娩复杂的发生率也明显高于多产妇。首先根据生育次数和既往分娩方式对产妇进行分组,然后在这些组内根据具体危险因素的存在情况进行分组,这将为产妇提供更大、更明智的选择,更有针对性地进行干预,并减少分娩过程中的转移,优于仅根据危险因素进行分组。