Asamoah Francis Adumata, Yarney Joel, Scott Aba, Vanderpuye Verna, Yuan Zhigang, Fernandez Daniel C, Montejo Michael E, Agyeman Mervin, Boateng Samuel Ntiamoah, Anarfi Kwabena, Aidoo Charles, Shahzad Mian M, Chern Jing-Yi, Chon Hye-Sook, Wenham Robert M, Yamoah Kosj, Ahmed Kamran A
Department of Radiation Oncology, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL.
National Radiotherapy Oncology and Nuclear Medicine Center of the Korle-Bu Teaching Hospital, Accra, Ghana.
JCO Glob Oncol. 2020 Oct;6:1510-1518. doi: 10.1200/GO.20.00303.
Cervical cancer remains a major health challenge in low- to middle-income countries. We present the experiences of two centers practicing in variable resource environments to determine predictors of improved radiochemotherapy treatment.
This comparative review describes cervical cancer presentation and treatment with concurrent chemoradiotherapy with high-dose-rate brachytherapy between 2014 and 2017 at the National Radiotherapy Oncology and Nuclear Medicine Center (NRONMC) in Korle-Bu Teaching Hospital, Accra, Ghana, and Moffitt Cancer Center (MCC), Tampa, FL.
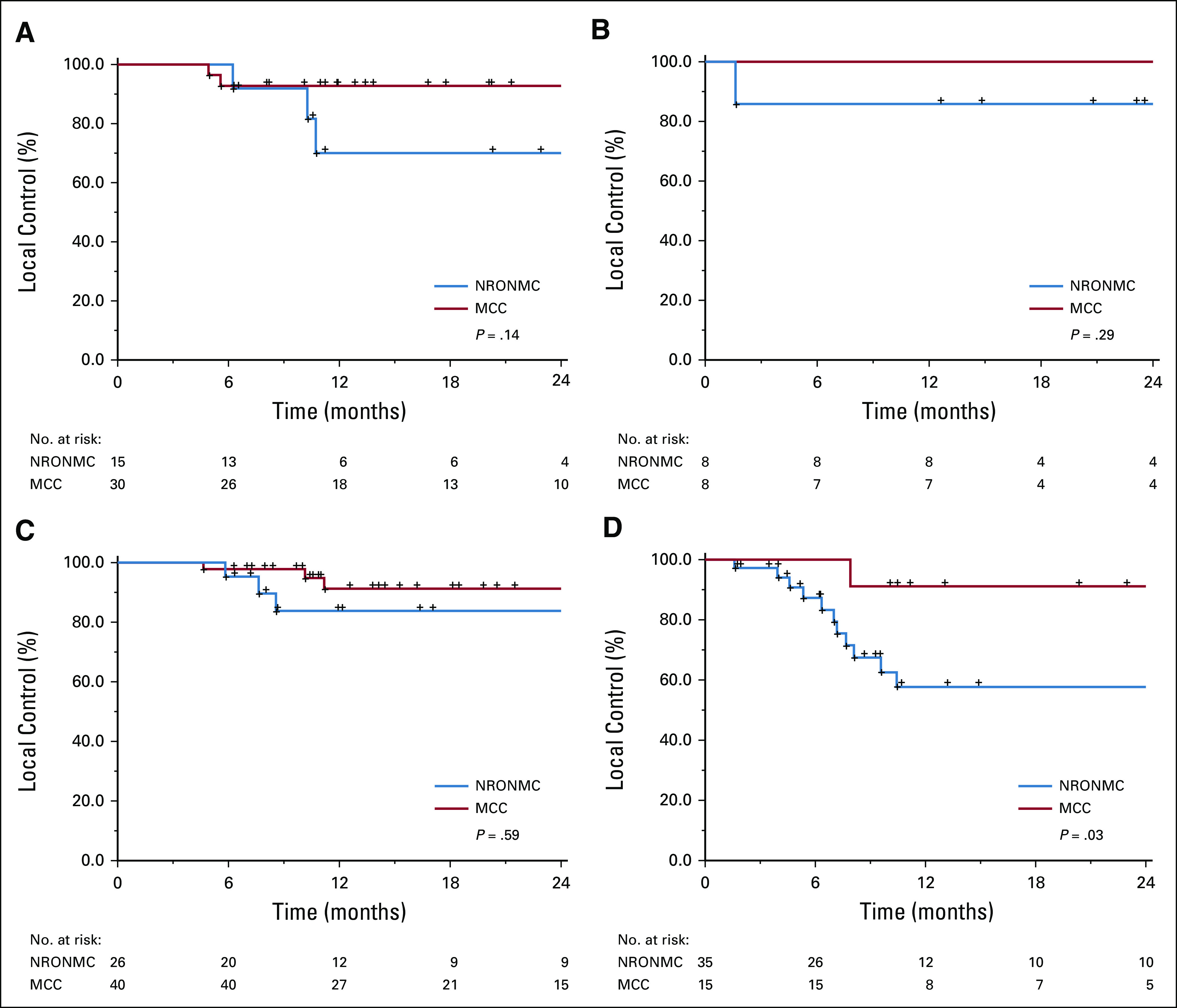
Median follow-up for this study was 16.9 months. NRONMC patients presented with predominantly stage III disease (42% 16%; = .002). MCC patients received para-aortic node irradiation (16%) and interstitial brachytherapy implants (19%). Median treatment duration was longer for NRONMC patients compared with MCC patients (59 52 days; < .0001), and treatment duration ≥ 55 days predicted worse survival on multivariable analysis (MVA; = .02). Stage ≥ III disease predicted poorer local control on MVA. There was a difference in local control among patients with stage III disease (58% 91%; = .03) but not in survival between MCC and NRONMC. No significant difference in local control was observed for stage IB, IIA, and IIB disease.
Although there were significant differences in disease presentation between the two centers, treatment outcomes were similar for patients with early-stage disease. Longer treatment duration and stage ≥ III disease predicted poor outcomes.
在低收入和中等收入国家,宫颈癌仍然是一项重大的健康挑战。我们介绍了两个在不同资源环境下开展业务的中心的经验,以确定改善放化疗治疗效果的预测因素。
本比较性综述描述了2014年至2017年期间,加纳阿克拉科尔勒-布教学医院的国家放射肿瘤学与核医学中心(NRONMC)以及佛罗里达州坦帕市的莫菲特癌症中心(MCC)对宫颈癌患者进行同步放化疗及高剂量率近距离放疗的情况。
本研究的中位随访时间为16.9个月。NRONMC的患者主要表现为III期疾病(42%对16%;P = 0.002)。MCC的患者接受了腹主动脉旁淋巴结照射(16%)和组织间近距离放疗植入(19%)。与MCC的患者相比,NRONMC的患者中位治疗持续时间更长(59天对52天;P < 0.0001),多变量分析(MVA)显示治疗持续时间≥55天预示着生存情况较差(P = 0.02)。III期及以上疾病在MVA中预示着局部控制较差。III期疾病患者的局部控制存在差异(58%对91%;P = 0.03),但MCC和NRONMC患者的生存率无差异。对于IB、IIA和IIB期疾病,未观察到局部控制的显著差异。
尽管两个中心在疾病表现上存在显著差异,但早期疾病患者的治疗结果相似。较长的治疗持续时间和III期及以上疾病预示着预后较差。