Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht University, Utrecht, The Netherlands.
Department of Internal Medicine, School for Cardiovascular Diseases CARIM, Maastricht University Medical Centre+, Maastricht, The Netherlands.
BMJ Open Diabetes Res Care. 2020 Oct;8(1). doi: 10.1136/bmjdrc-2020-001365.
Sex differences in cardiometabolic risk factors and their management in type 2 diabetes (T2D) have not been fully identified. Therefore, we aimed to examine differences in cardiometabolic risk factor levels, pharmacological treatment and achievement of risk factor control between women and men with T2D.
Cross-sectional data from the Dutch Diabetes Pearl cohort were used (n=6637, 40% women). Linear and Poisson regression analyses were used to examine sex differences in cardiometabolic risk factor levels, treatment, and control.
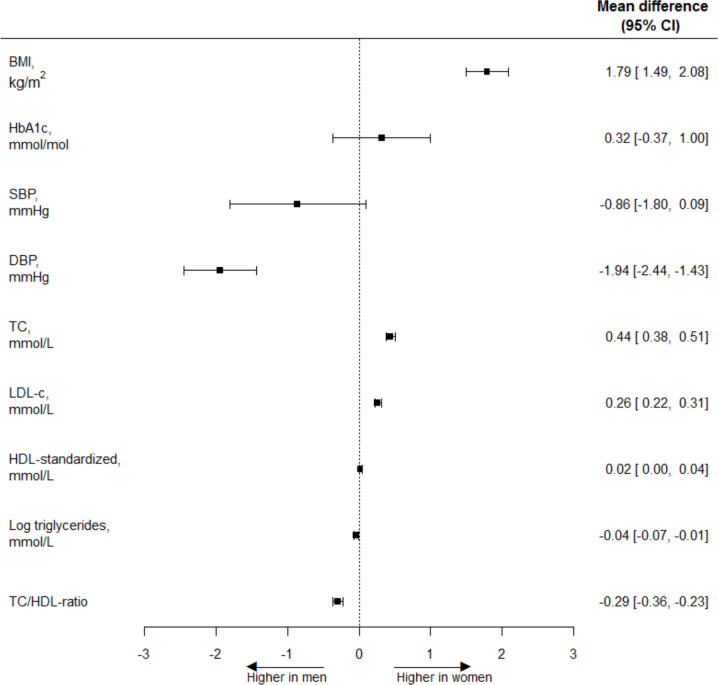
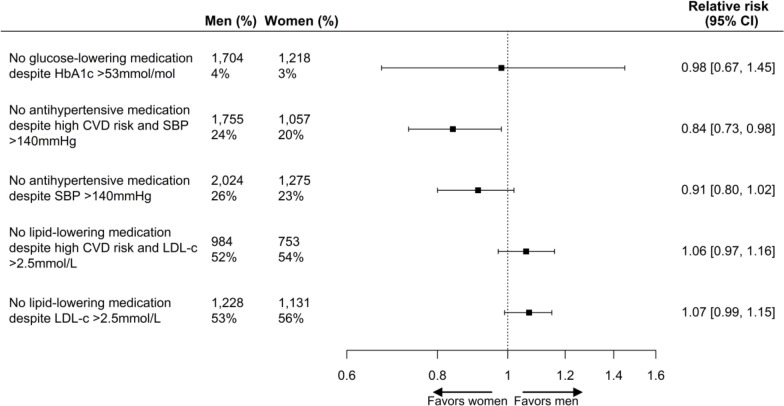
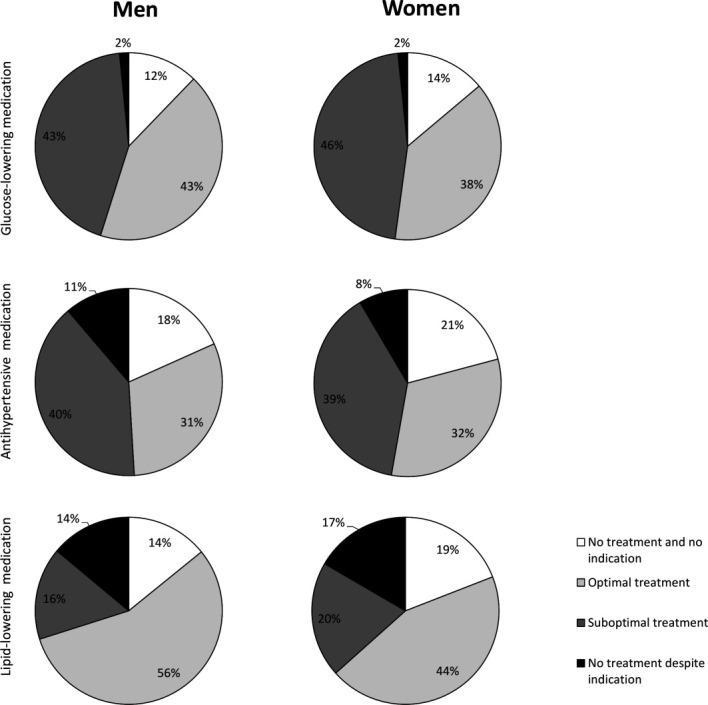
Compared with men, women had a significantly higher body mass index (BMI) (mean difference 1.79 kg/m (95% CI 1.49 to 2.08)), while no differences were found in hemoglobin A (HbA) and systolic blood pressure (SBP). Women had lower diastolic blood pressure (-1.94 mm Hg (95% CI -2.44 to -1.43)), higher total cholesterol (TC) (0.44 mmol/L (95% CI 0.38 to 0.51)), low-density lipoprotein cholesterol (LDL-c) (0.26 mmol/L (95% CI 0.22 to 0.31)), and high-density lipoprotein cholesterol (HDL-c) sex-standardized (0.02 mmol/L (95% CI 0.00 to 0.04)), and lower TC:HDL ratio (-0.29 (95% CI -0.36 to -0.23)) and triglycerides (geometric mean ratio 0.91 (95% CI 0.85 to 0.98)). Women had a 16% higher probability of being treated with antihypertensive medication in the presence of high cardiovascular disease (CVD) risk and elevated SBP than men (relative risk 0.84 (95% CI 0.73 to 0.98)), whereas no sex differences were found for glucose-lowering medication and lipid-modifying medication. Among those treated, women were less likely to achieve treatment targets of HbA (0.92 (95% CI 0.87 to 0.98)) and LDL-c (0.89 (95% CI 0.85 to 0.92)) than men, while no differences for SBP were found.
In this Dutch T2D population, women had a slightly different cardiometabolic risk profile compared with men and a substantially higher BMI. Women had a higher probability of being treated with antihypertensive medication in the presence of high CVD risk and elevated SBP than men, and were less likely than men to achieve treatment targets for HbA and LDL levels.
2 型糖尿病(T2D)患者的心血管代谢风险因素及其管理方面的性别差异尚未完全明确。因此,我们旨在研究女性和男性 T2D 患者的心血管代谢风险因素水平、药物治疗以及风险因素控制方面的差异。
使用荷兰糖尿病珍珠队列的横断面数据(n=6637,40%为女性)。采用线性和泊松回归分析来研究心血管代谢风险因素水平、治疗和控制方面的性别差异。
与男性相比,女性的体重指数(BMI)明显更高(平均差值 1.79kg/m2(95%置信区间 1.49 至 2.08)),而血红蛋白 A(HbA)和收缩压(SBP)无差异。女性的舒张压较低(-1.94mmHg(95%置信区间-2.44 至-1.43)),总胆固醇(TC)较高(0.44mmol/L(95%置信区间 0.38 至 0.51))、低密度脂蛋白胆固醇(LDL-c)较高(0.26mmol/L(95%置信区间 0.22 至 0.31))、高密度脂蛋白胆固醇(HDL-c)标准化后较高(0.02mmol/L(95%置信区间 0.00 至 0.04)),且 TC:HDL 比值较低(-0.29(95%置信区间-0.36 至-0.23))和甘油三酯较低(几何均数比值 0.91(95%置信区间 0.85 至 0.98))。女性在存在高心血管疾病(CVD)风险和升高的 SBP 时,使用降压药物治疗的可能性比男性高 16%(相对风险 0.84(95%置信区间 0.73 至 0.98)),而在血糖降低药物和血脂调节药物方面没有性别差异。在接受治疗的患者中,女性达到 HbA(0.92(95%置信区间 0.87 至 0.98))和 LDL-c(0.89(95%置信区间 0.85 至 0.92))治疗目标的可能性低于男性,而 SBP 则没有差异。
在荷兰 T2D 人群中,女性的心血管代谢风险特征与男性略有不同,且 BMI 略高。女性在存在高 CVD 风险和升高的 SBP 时,使用降压药物治疗的可能性比男性高,且达到 HbA 和 LDL 水平治疗目标的可能性低于男性。