Brar Gagandeep, Greten Tim F, Graubard Barry I, McNeel Timothy S, Petrick Jessica L, McGlynn Katherine A, Altekruse Sean F
Gastrointestinal Malignancy Section Thoracic and Gastrointestinal Malignancies Branch Center for Cancer Research National Cancer Institute National Institutes of Health Bethesda MD.
Present address: Department of Hematology and Oncology Weill Cornell Medical College New York NY.
Hepatol Commun. 2020 Aug 9;4(10):1541-1551. doi: 10.1002/hep4.1564. eCollection 2020 Oct.
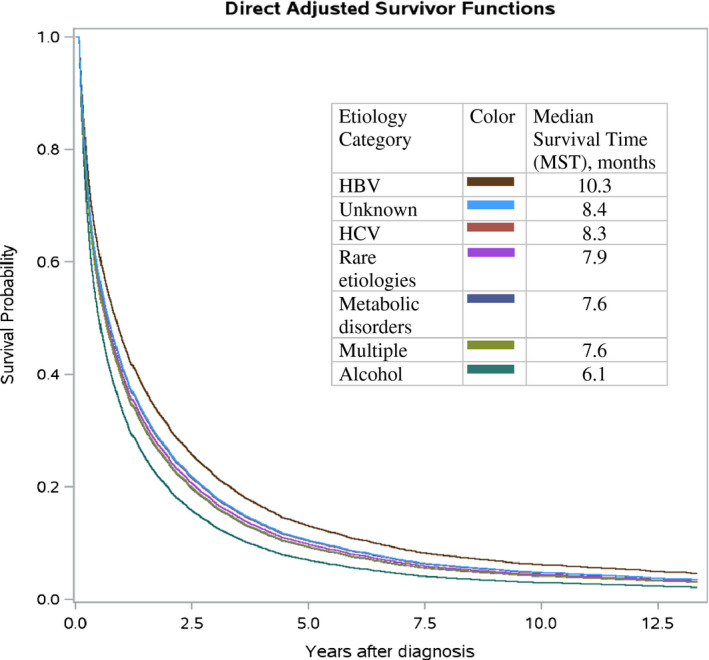
In the United States, hepatocellular carcinoma (HCC) survival varies with tumor characteristics, patient comorbidities, and treatment. The effect of HCC etiology on survival is less clearly defined. The relationship between HCC etiology and mortality was examined using Surveillance, Epidemiology, and End Results-Medicare data. In a cohort of 11,522 HCC cases diagnosed from 2000 through 2014, etiologies were identified from Medicare data, including metabolic disorders (32.9%), hepatitis C virus (8.2%), alcohol (4.7%), hepatitis B virus (HBV, 2.1%), rare etiologies (0.9%), multiple etiologies (26.7%), and unknown etiology (24.4%). After adjusting for demographics, tumor characteristics, comorbidities and treatment, hazard ratios (HRs) and survival curves by HCC etiology were estimated using Cox proportional hazard models. Compared with HBV-related HCC cases, higher mortality was observed for those with alcohol-related HCC (HR 1.49; 95% confidence interval [95% CI] 1.25-1.77), metabolic disorder-related HCC (HR 1.25; 95% CI 1.07-1.47), and multiple etiology-related HCC (HR 1.25; 95% CI 1.07-1.46), but was not statistically significant for hepatitis C virus-related, rare disorder-related, and HCC of unknown etiology. For all HCC etiologies, there was short median survival ranging from 6.1 months for alcohol to 10.3 months for HBV. More favorable survival was seen with HBV-related HCC. To the extent that HCC screening is more common among persons with HBV infection compared to those with other etiologic risk factors, population-based HCC screening, applied evenly to persons across all HCC etiology categories, could shift HCC diagnosis to earlier stages, when cases with good clinical status are more amenable to curative therapy.
在美国,肝细胞癌(HCC)患者的生存率因肿瘤特征、患者合并症及治疗方式而异。HCC病因对生存率的影响尚不太明确。本研究利用监测、流行病学及最终结果-医疗保险数据,探讨了HCC病因与死亡率之间的关系。在2000年至2014年间确诊的11522例HCC病例队列中,从医疗保险数据中确定病因,包括代谢紊乱(32.9%)、丙型肝炎病毒(8.2%)、酒精(4.7%)、乙型肝炎病毒(HBV,2.1%)、罕见病因(0.9%)、多种病因(26.7%)及病因不明(24.4%)。在对人口统计学、肿瘤特征、合并症及治疗进行校正后,使用Cox比例风险模型估计不同HCC病因的风险比(HR)及生存曲线。与HBV相关的HCC病例相比,酒精相关HCC(HR 1.49;95%置信区间[95%CI] 1.25-1.77)、代谢紊乱相关HCC(HR 1.25;95%CI 1.07-1.47)及多种病因相关HCC(HR 1.25;95%CI 1.07-1.46)患者的死亡率更高,但丙型肝炎病毒相关、罕见疾病相关及病因不明的HCC患者死亡率差异无统计学意义。所有HCC病因的中位生存期均较短,酒精相关HCC为6.1个月,HBV相关HCC为10.3个月。HBV相关HCC患者的生存率更优。鉴于与其他病因风险因素患者相比,HBV感染患者中HCC筛查更为普遍,对所有HCC病因类别的人群均一应用基于人群的HCC筛查,可能会将HCC诊断提前至临床状态良好、更适合进行根治性治疗的早期阶段。