Johnson Philip, Berhane Sarah, Kagebayashi Chiaki, Satomura Shinji, Teng Mabel, Fox Richard, Yeo Winnie, Mo Frankie, Lai Paul, Chan Stephen L, Tada Toshifumi, Toyoda Hidenori, Kumada Takashi
Department of Molecular and Clinical Cancer Medicine, University of Liverpool and Clatterbridge Cancer Centre NHS Foundation Trust, Sherrington Building, Ashton Street, Liverpool, Merseyside L69 3GA, UK.
The Clatterbridge Cancer Centre NHS Foundation Trust, Clatterbridge Road, Bebington, Wirral CH63 4JY, UK.
Br J Cancer. 2017 Feb 14;116(4):441-447. doi: 10.1038/bjc.2016.422. Epub 2017 Jan 12.
Variation in survival in hepatocellular carcinoma (HCC) has been attributed to different aetiologies or disease stages at presentation. While international guidelines recommend surveillance of high-risk groups to permit early diagnosis and curative treatment, the evidence that surveillance decreases disease-specific mortality is weak.
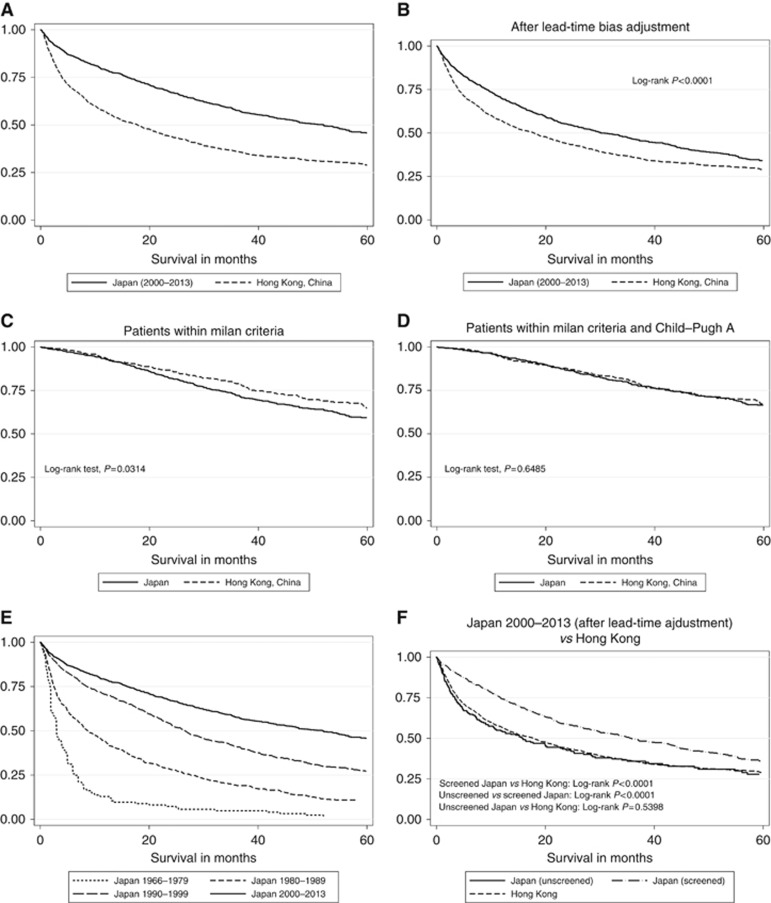
We compared HCC survival figures from Japan (n=1174) and Hong Kong (n=1675) over similar time periods (Japan 2000-2013, Hong Kong, China 2003-2014). The former has an intensive national surveillance programme, while the latter has none. We also analysed changes in survival in Japan over a 50-year period including data from before and after institution of a national HCC surveillance programme.
In Japan, over 75% of cases are currently detected by surveillance, whereas in Hong Kong <20% of cases are detected presymptomatically. Median survival was 52 months in Japan and 17.8 months in Hong Kong; this survival advantage persisted after allowance for lead-time bias. Sixty-two per cent of Japanese patients had early disease at diagnosis and 63% received curative treatment. The comparable figures for Hong Kong were 31.7% and 44.1%, respectively. These differences could not be accounted for by disease aetiology, and patients in Hong Kong who were detected at an early stage had a similar survival to the analogous patients in Japan.
The variation in survival is largely accounted for by stage at diagnosis, which in turn relates to the intensity of surveillance programmes and the consequent variation in curative therapeutic options.
肝细胞癌(HCC)患者生存率的差异归因于发病时不同的病因或疾病阶段。尽管国际指南建议对高危人群进行监测以实现早期诊断和根治性治疗,但监测可降低疾病特异性死亡率的证据并不充分。
我们比较了日本(n = 1174)和中国香港(n = 1675)在相似时间段(日本为2000 - 2013年,中国香港为2003 - 2014年)的HCC生存数据。前者有一项全国性的密集监测计划,而后者没有。我们还分析了日本50年间的生存变化情况,包括全国HCC监测计划实施前后的数据。
在日本,目前超过75%的病例是通过监测发现的,而在中国香港,只有不到20%的病例是在出现症状前被发现的。日本的中位生存期为52个月,中国香港为17.8个月;在考虑了领先时间偏倚后,这种生存优势依然存在。62%的日本患者在诊断时处于疾病早期,63%接受了根治性治疗。中国香港的相应数字分别为31.7%和44.1%。这些差异无法用疾病病因来解释,在中国香港早期被发现的患者与日本类似患者的生存期相似。
生存率的差异很大程度上是由诊断时的疾病阶段造成的,而这又与监测计划的强度以及随之而来的根治性治疗选择的差异有关。