Population Health Research Institute, St George's, University of London, UK.
Population Health Research Institute, St George's, University of London, UK.
Environ Int. 2020 Nov;144:105998. doi: 10.1016/j.envint.2020.105998. Epub 2020 Oct 5.
WHO has published several volumes of Global Air Quality Guidelines to provide guidance on the health risks associated with exposure to outdoor air pollution. As new scientific evidence is generated, air quality guidelines need to be periodically revised and, where necessary, updated.
The aims of the study were 1) to summarise the available evidence on the effect of long-term exposure to ozone (O) and nitrogen dioxide (NO) on mortality; 2) and to assess concentration response functions (CRF), their shape and the minimum level of exposures measured in studies to support WHO's update of the global air quality guidelines.
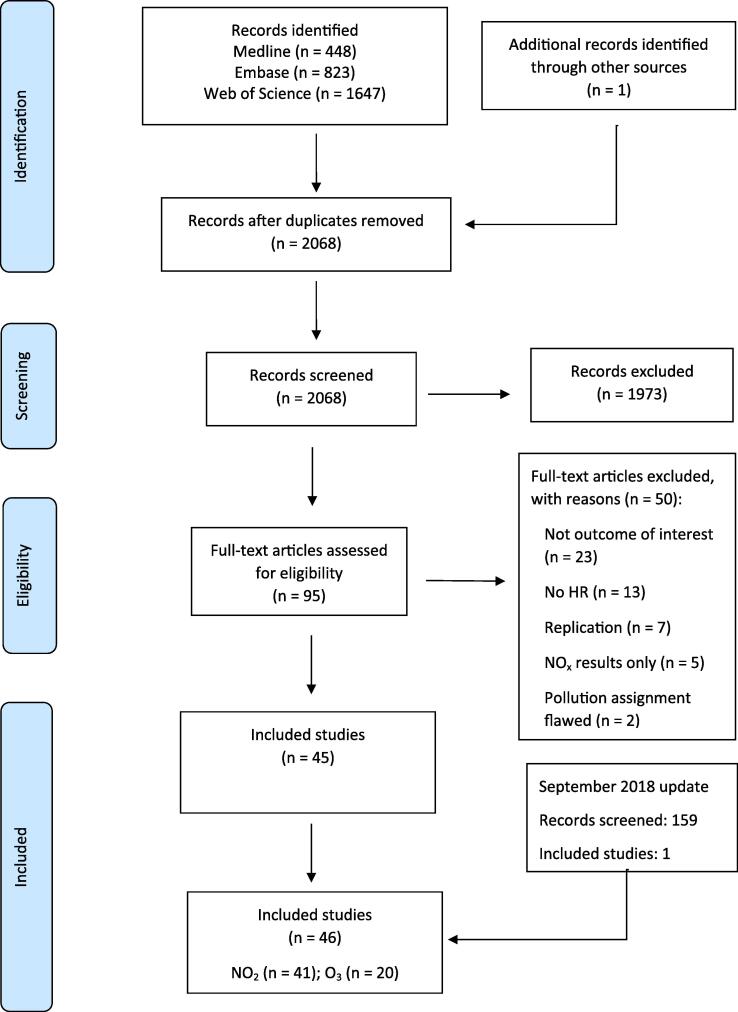
We conducted a systematic literature search of the Medline, Embase and Web of Science databases following a protocol proposed by WHO and applied Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines for reporting our results.
Cohort studies in human populations (including sub-groups at risk) exposed to long-term concentrations of NO and O. Outcomes assessed were all-cause, respiratory, Chronic Obstructive Pulmonary Disease (COPD) and Acute Lower Respiratory Infection (ALRI) mortality.
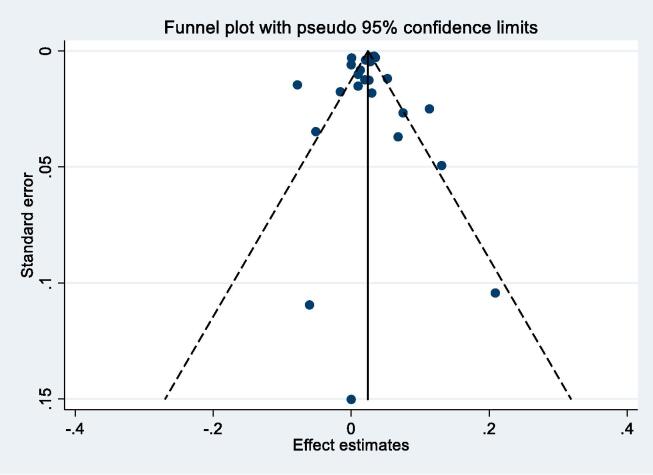
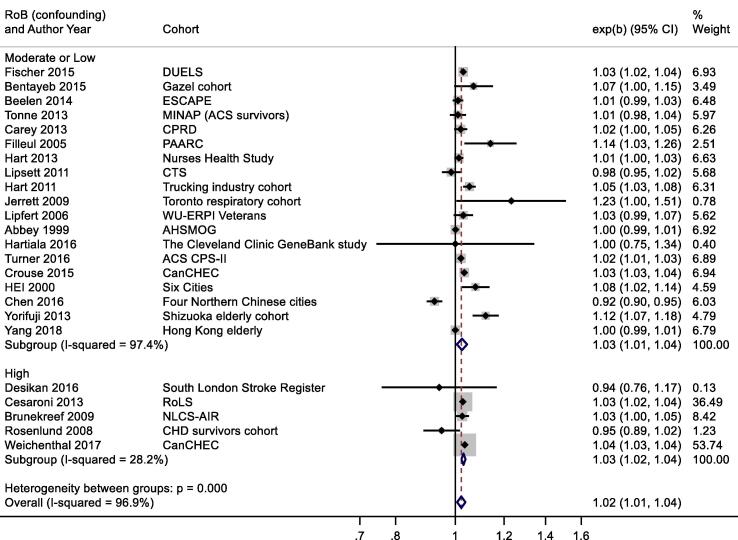
Studies included in the meta-analyses were assessed using a new Risk of Bias instrument developed by a group of experts convened by WHO. Study results are presented in forest plots and quantitative meta-analyses were conducted using random effects models. The certainty of evidence was assessed using a newly developed adaptation of GRADE.
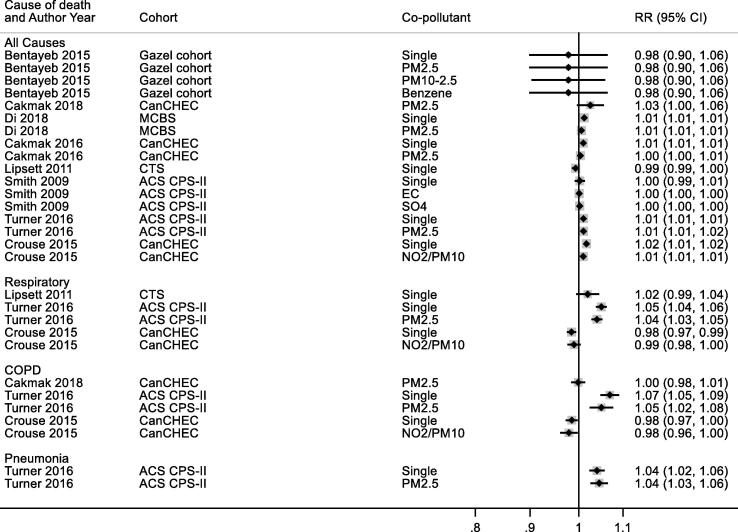
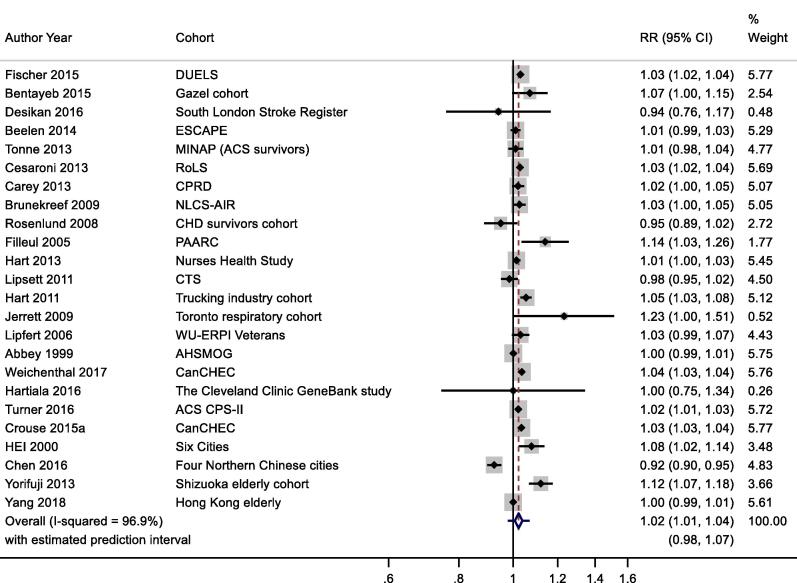
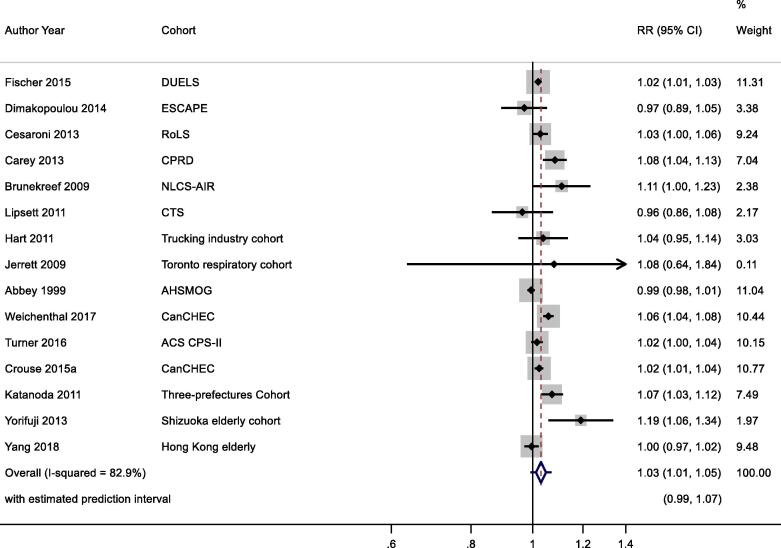
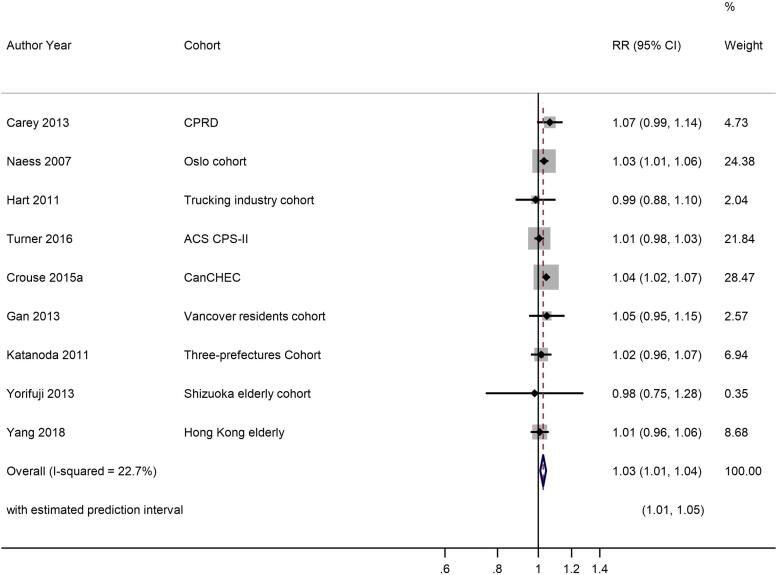
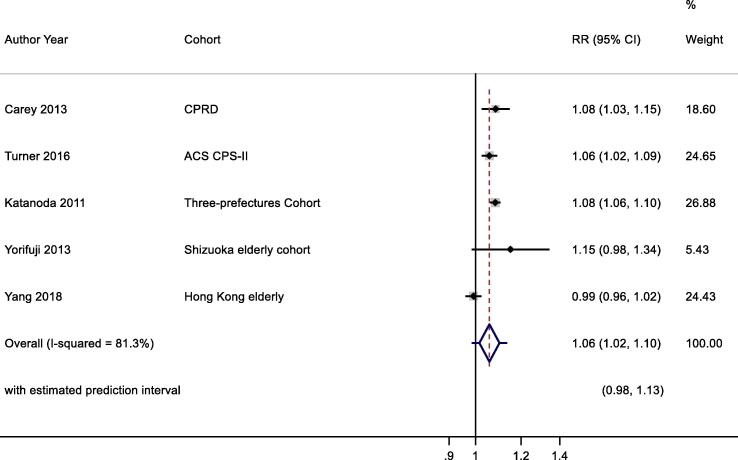
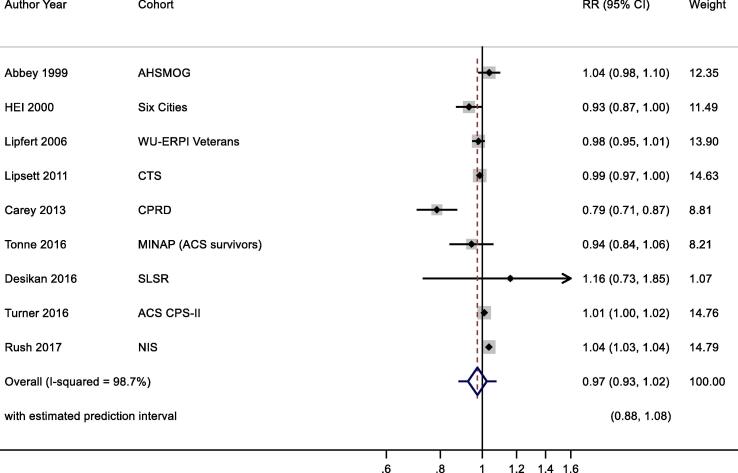
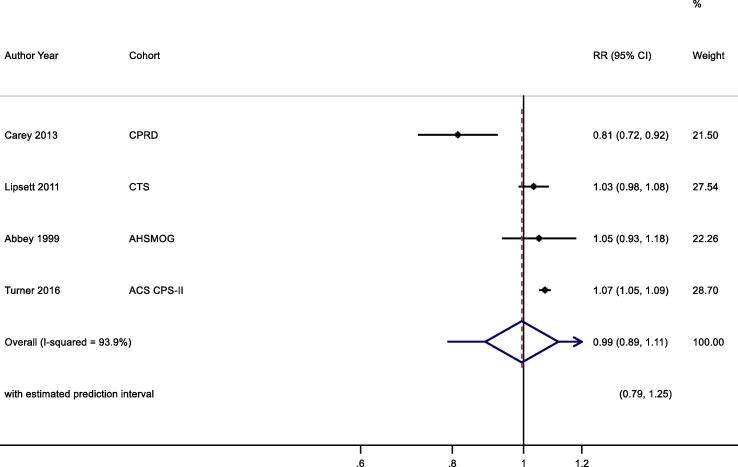
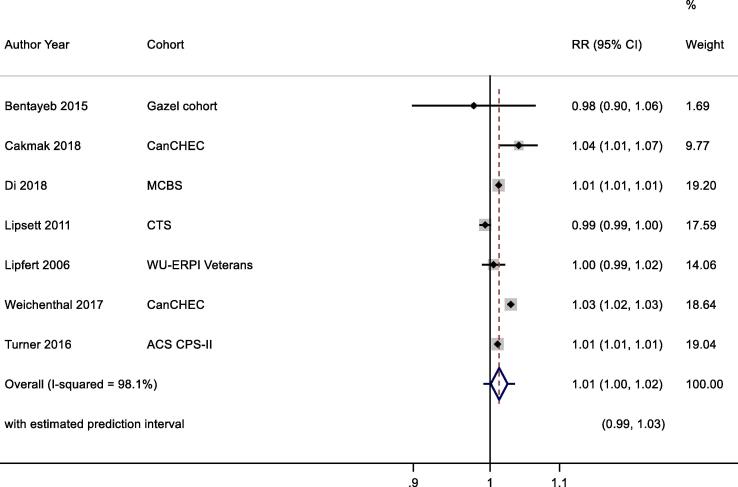
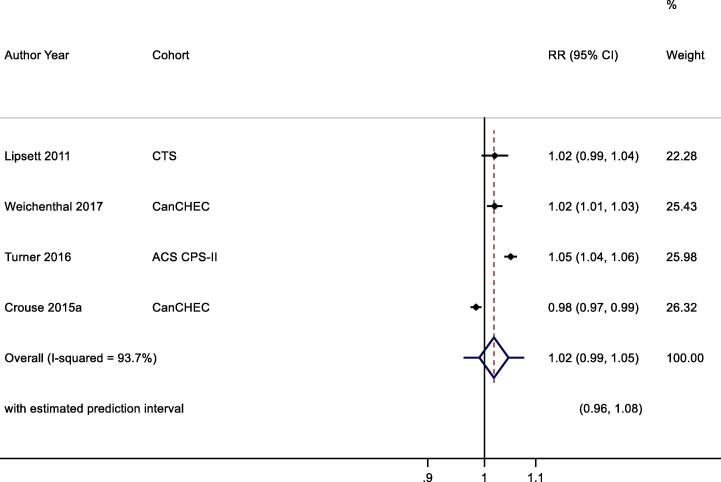
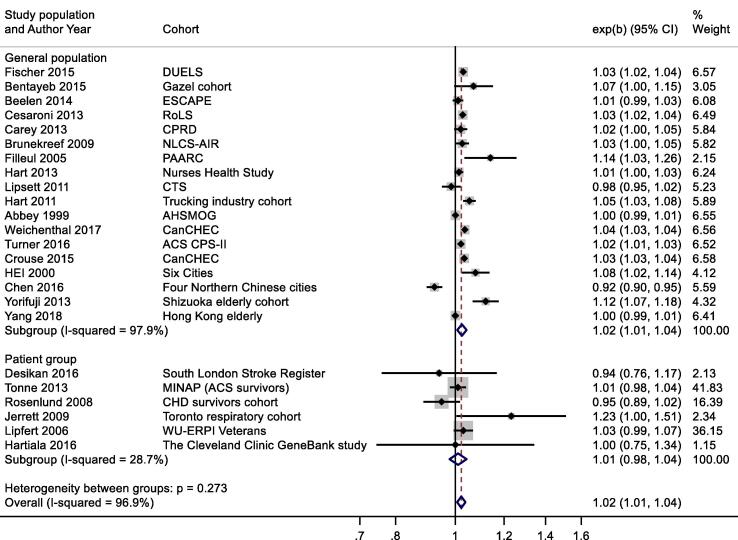
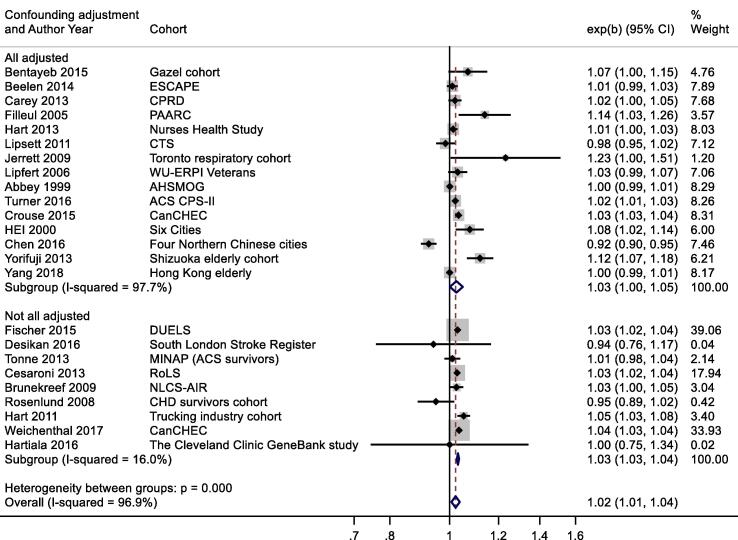
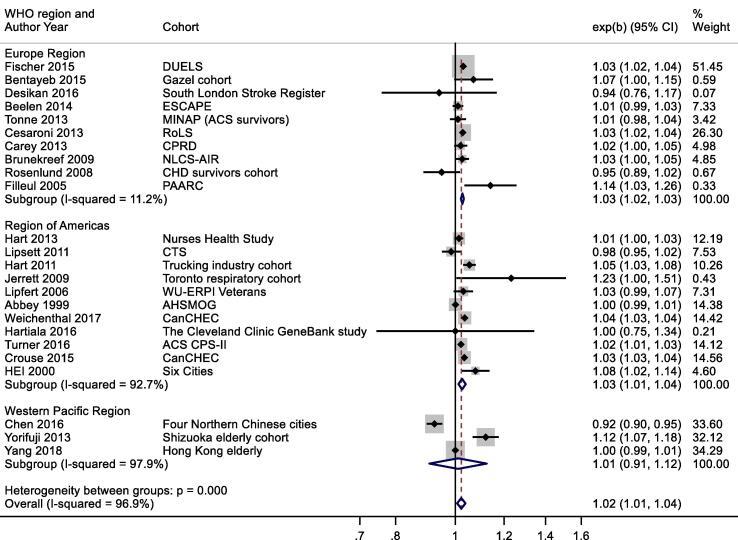
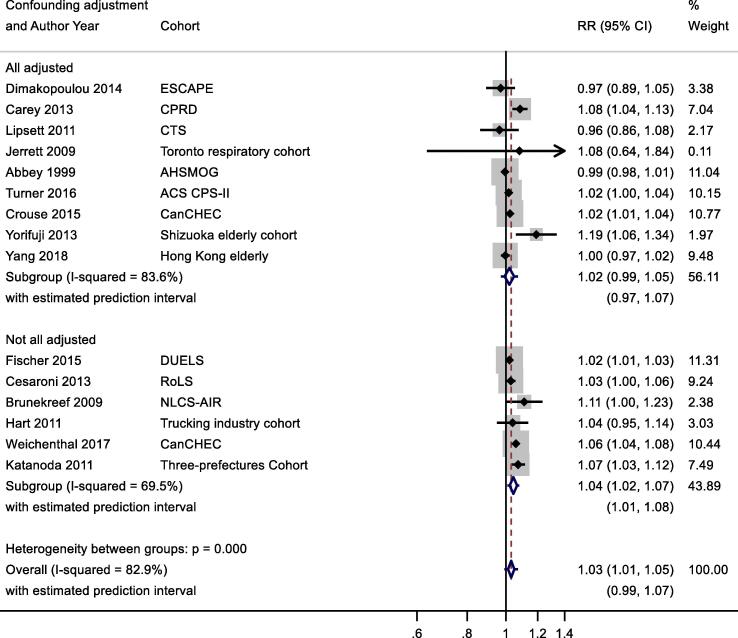
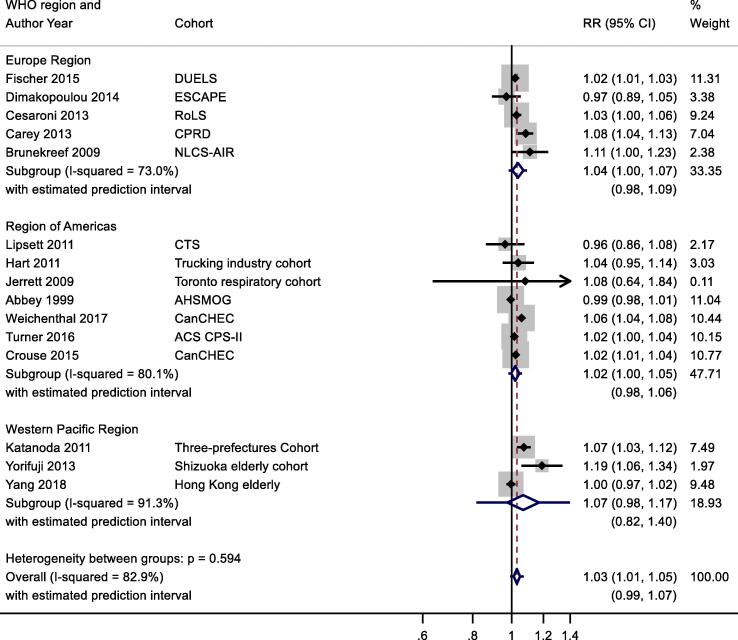
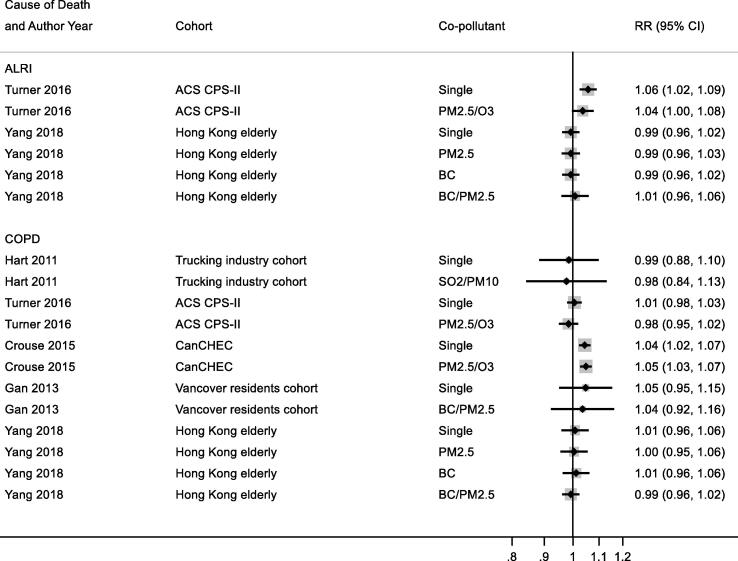
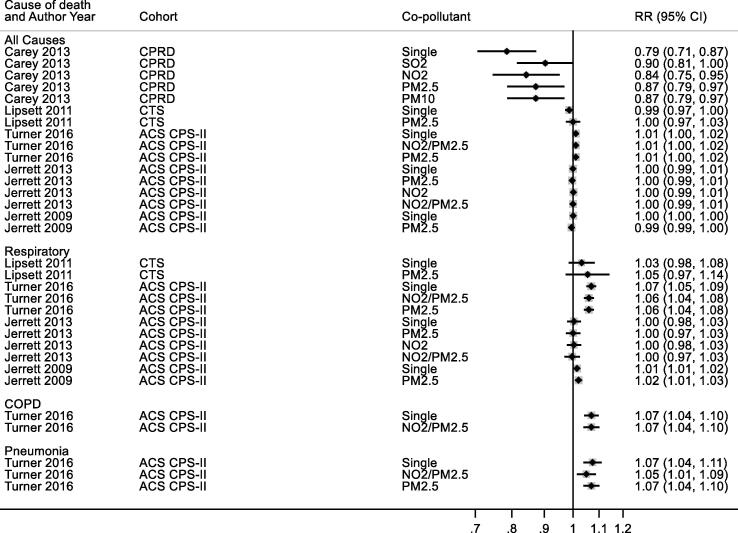
The review identified 2068 studies of which 95 were subject to full-text review with 45 meeting the inclusion criteria. An update in September 2018 identified 159 studies with 1 meeting the inclusion criteria. Of the 46 included studies, 41 reported results for NO and 20 for O. The majority of studies were from the USA and Europe with the remainder from Canada, China and Japan. Forty-two studies reported results for all-cause mortality and 22 for respiratory mortality. Associations for NO and mortality were positive; random-effects summary relative risks (RR) were 1.02 (95% CI: 1.01, 1.04), 1.03 (1.00, 1.05), 1.03 (1.01, 1.04) and 1.06 (1.02, 1.10) per 10 μg/m for all-cause (24 cohorts), respiratory (15 cohorts), COPD (9 cohorts) and ALRI (5 cohorts) mortality respectively. The review identified high levels of heterogeneity for all causes of death except COPD. A small number of studies investigated the shape of the concentration-response relationship and generally found little evidence to reject the assumption of linearity across the concentration range. Studies of O using annual metrics showed the associations with all-cause and respiratory mortality were 0.97 (0.93, 1.02) and 0.99 (0.89, 1.11) per 10 μg/m respectively. For studies using peak O metrics, the association with all-cause mortality was 1.01 (1.00, 1.02) and for respiratory mortality 1.02 (0.99, 1.05), each per 10 μg/m. The review identified high levels of heterogeneity. Few studies investigated the shape of the concentration-response relationship. Certainty in the associations (adapted GRADE) with mortality was rated low to moderate for each exposure-outcome pair, except for NO and COPD mortality which was rated high.
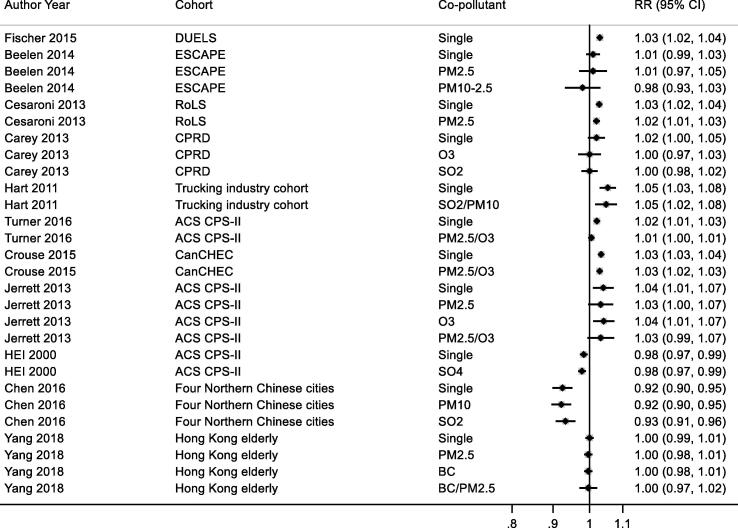
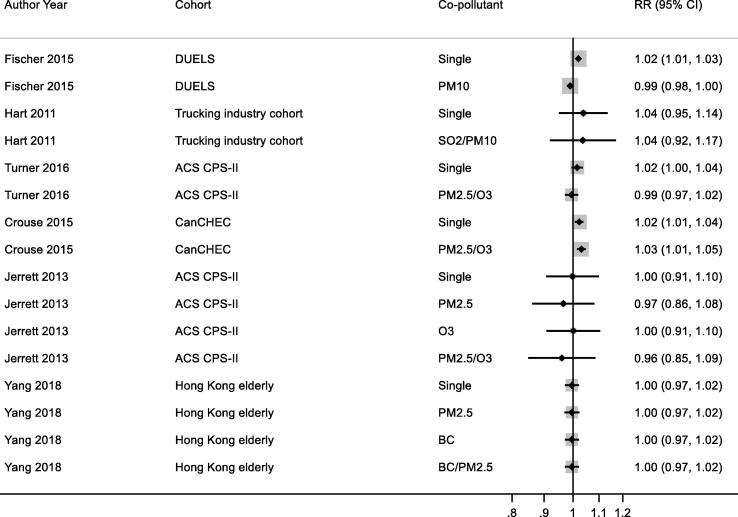
The substantial heterogeneity for most outcomes in the review requires explanation. The evidence base is limited in terms of the geographical spread of the study populations and, for some outcomes, the small number of independent cohorts for meta-analysis precludes meaningful meta-regression to explore causes of heterogeneity. Relatively few studies assessed specifically the shape of the CRF or multi-pollutant models.
The short-comings in the existing literature base makes determining the precise nature (magnitude and linearity) of the associations challenging. Certainty of evidence assessments were moderate or low for both NO and O for all causes of mortality except for NO and COPD mortality where the certainty of the evidence was judged as high.
世界卫生组织已经发布了几卷《全球空气质量指南》,旨在提供有关接触户外空气污染与健康风险相关的指导。随着新的科学证据不断涌现,空气质量指南需要定期修订,并在必要时进行更新。
本研究的目的是 1)总结长期暴露于臭氧(O)和二氧化氮(NO)对死亡率的影响的现有证据;2)评估浓度反应函数(CRF)、其形状以及支持世卫组织更新全球空气质量指南的研究中测量的最低暴露水平。
我们按照世卫组织提出的方案对 Medline、Embase 和 Web of Science 数据库进行了系统文献检索,并按照系统评价和荟萃分析的首选报告项目(PRISMA)指南报告了研究结果。
在长期接触 NO 和 O 的情况下,人类人群(包括高危亚群)的队列研究。评估的结果是全因、呼吸、慢性阻塞性肺疾病(COPD)和急性下呼吸道感染(ALRI)死亡率。
使用由世卫组织召集的一组专家制定的新的风险偏差工具评估纳入荟萃分析的研究。研究结果以森林图呈现,并使用随机效应模型进行定量荟萃分析。使用新开发的 GRADE 改编版评估证据的确定性。
该综述共确定了 2068 项研究,其中 95 项进行了全文审查,其中 45 项符合纳入标准。2018 年 9 月的更新确定了 159 项研究,其中 1 项符合纳入标准。在 46 项纳入的研究中,41 项报告了 NO 的结果,20 项报告了 O 的结果。大多数研究来自美国和欧洲,其余研究来自加拿大、中国和日本。42 项研究报告了全因死亡率的结果,22 项研究报告了呼吸死亡率的结果。NO 和死亡率之间的关联为阳性;随机效应汇总相对风险(RR)分别为 1.02(95% CI:1.01,1.04)、1.03(1.00,1.05)、1.03(1.01,1.04)和 1.06(1.02,1.10)每 10μg/m3 用于全因(24 个队列)、呼吸(15 个队列)、COPD(9 个队列)和 ALRI(5 个队列)死亡率。除 COPD 外,所有死因的异质性水平均较高。少数研究调查了浓度反应关系的形状,通常发现几乎没有证据可以否定浓度范围内线性关系的假设。使用年度指标的 O 研究表明,全因和呼吸死亡率与 O 的关联分别为 0.97(0.93,1.02)和 0.99(0.89,1.11)每 10μg/m3。对于使用峰 O 指标的研究,全因死亡率的关联为 1.01(1.00,1.02),呼吸死亡率的关联为 1.02(0.99,1.05),每 10μg/m3。该综述的异质性水平较高。很少有研究调查浓度反应关系的形状。对于每个暴露-结果组合,与死亡率相关的关联的确定性(改编后的 GRADE)被评为低到中度,除了 NO 和 COPD 死亡率被评为高。
该综述中大多数结果的高度异质性需要解释。从研究人群的地理分布来看,证据基础有限,对于某些结果,元分析的独立队列数量较少,无法进行有意义的元回归来探索异质性的原因。相对较少的研究专门评估了 CRF 或多污染物模型的形状。
现有文献基础的不足之处使得确定关联的确切性质(幅度和线性)具有挑战性。对于全因死亡率,NO 和 O 的证据确定性评估为中度或低度,除了 NO 和 COPD 死亡率被评为高度。