Division of Radiology and Nuclear Medicine, Section of Paediatric Radiology, Oslo University Hospital, Oslo, Norway.
Department of Radiology and Clinical Physiology, Queen Silvia Children's Hospital, Sahlgrenska University Hospital, Rondv 10, S-41615, Göteborg, Sweden.
Pediatr Radiol. 2021 Jan;51(1):66-76. doi: 10.1007/s00247-020-04805-y. Epub 2020 Oct 9.
Children with Fontan circulation are at risk of developing hepatic fibrosis/cirrhosis. Reliable noninvasive monitoring techniques are lacking or under development.
To investigate surrogate indicators of hepatic fibrosis in adolescents with Fontan circulation by evaluating hepatic magnetic resonance (MR) T1 mapping and extracellular volume fraction measurements compared to US shear-wave elastography.
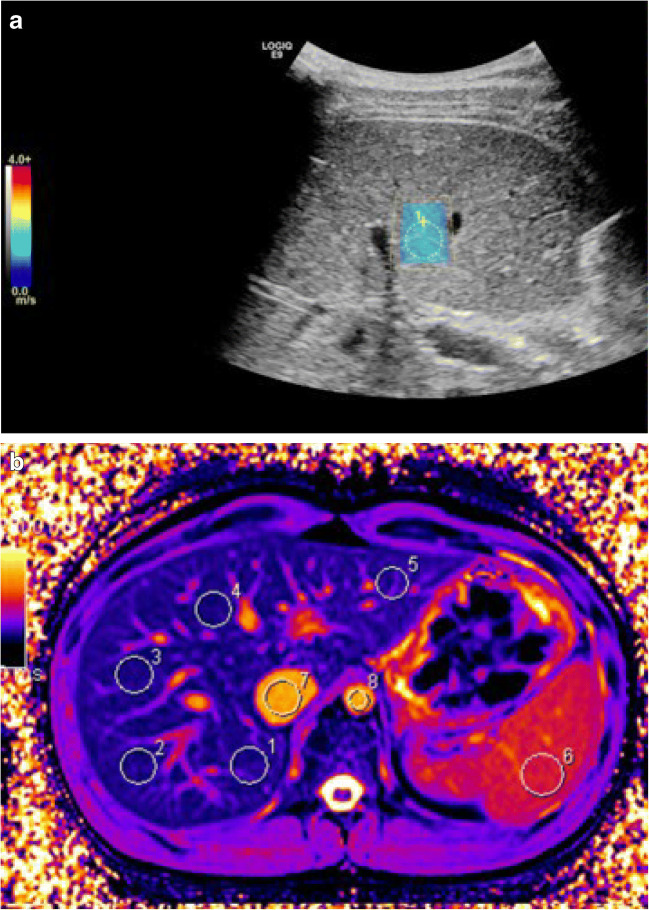
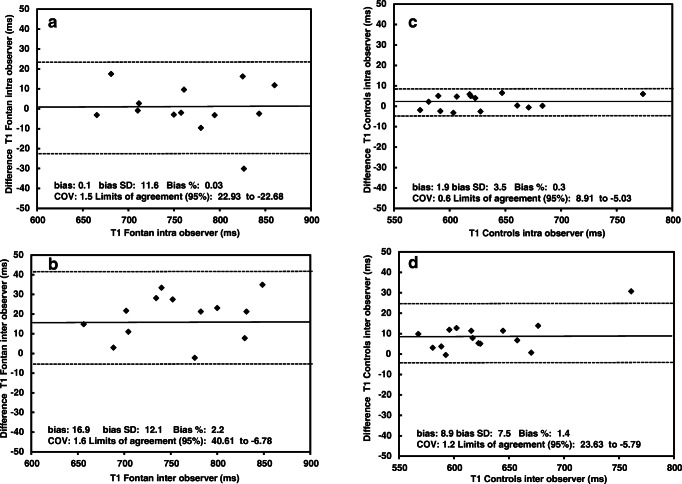
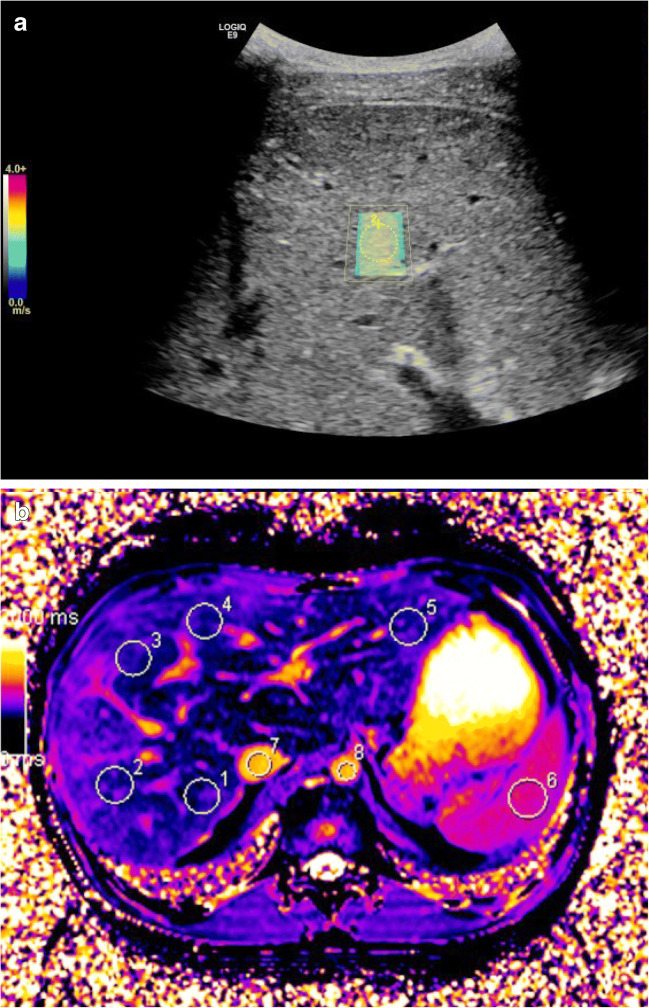
We analyzed hepatic native T1 times and extracellular volume fractions with modified Look-Locker inversion recovery. Liver stiffness was analyzed with shear-wave elastography. We compared results between 45 pediatric patients ages 16.7±0.6 years with Fontan circulation and 15 healthy controls ages 19.2±1.2 years. Measurements were correlated to clinical and hemodynamic data from cardiac catheterization.
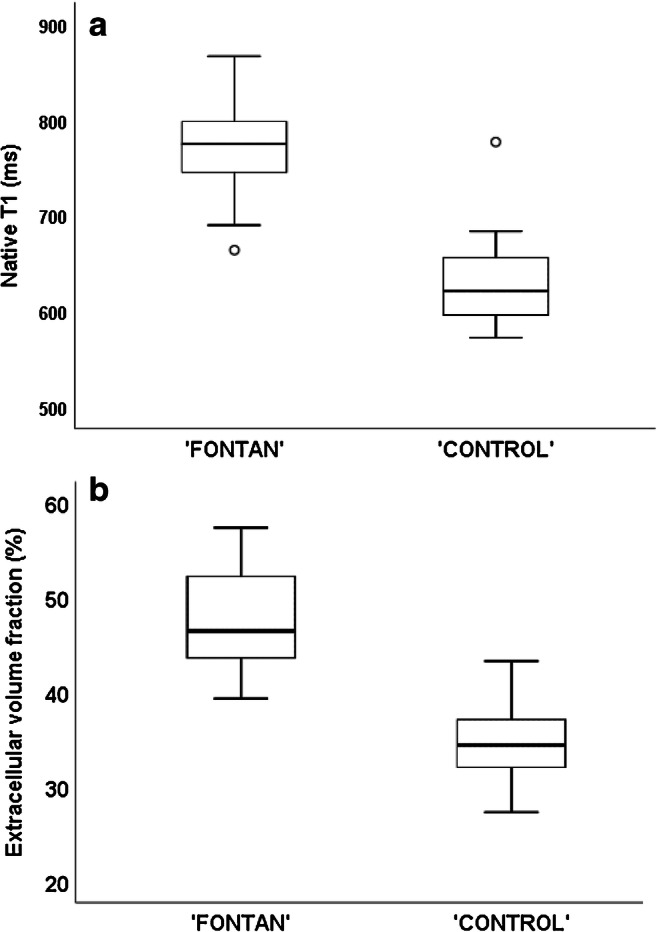
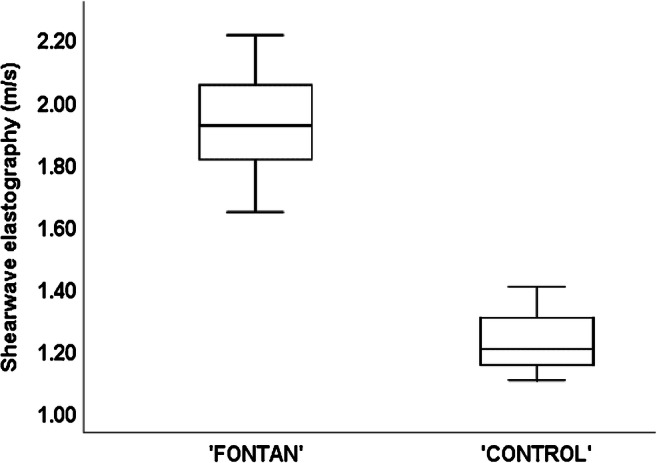
MR mapping was successful in 35/45 patients, revealing higher hepatic T1 times (774±44 ms) than in controls (632±52 ms; P<0.001) and higher extracellular volume fractions (47.4±5.0%) than in controls (34.6±3.8%; P<0.001). Liver stiffness was 1.91±0.13 m/s in patients vs. 1.20±0.10 m/s in controls (P<0.001). Native T1 times correlated with central venous pressures (r=0.5, P=0.007). Native T1 was not correlated with elastography in patients (r=0.2, P=0.1) or controls (r = -0.3, P=0.3). Extracellular volume fraction was correlated with elastography in patients (r=0.5, P=0.005) but not in controls (r=0.2, P=0.6).
Increased hepatic MR relaxometry and shear-wave elastography values in adolescents with Fontan circulation suggested the presence of hepatic fibrosis or congestion. Central venous pressure was related to T1 times. Changes were detected differently with MR relaxometry and elastography; thus, these techniques should not be used interchangeably in monitoring hepatic fibrosis.
Fontan 循环患儿有发生肝纤维化/肝硬化的风险。目前缺乏或正在开发可靠的非侵入性监测技术。
通过评估肝磁共振(MR)T1 映射和细胞外容积分数测量值,与超声剪切波弹性成像相比,研究 Fontan 循环青少年肝纤维化的替代指标。
我们分析了 45 名年龄为 16.7±0.6 岁的 Fontan 循环患儿和 15 名年龄为 19.2±1.2 岁的健康对照组的肝固有 T1 时间和细胞外容积分数,采用改良 Look-Locker 反转恢复法。采用剪切波弹性成像分析肝硬度。我们比较了 45 名 Fontan 循环患儿和 15 名健康对照组的结果。测量结果与心脏导管检查的临床和血流动力学数据相关。
35/45 例患者的 MR 成像成功,显示肝 T1 时间(774±44 ms)高于对照组(632±52 ms;P<0.001),细胞外容积分数(47.4±5.0%)高于对照组(34.6±3.8%;P<0.001)。患者的肝硬度为 1.91±0.13 m/s,对照组为 1.20±0.10 m/s(P<0.001)。固有 T1 时间与中心静脉压呈正相关(r=0.5,P=0.007)。在患者(r=0.2,P=0.1)或对照组(r = -0.3,P=0.3)中,固有 T1 与弹性成像均无相关性。细胞外容积分数与患者的弹性成像呈正相关(r=0.5,P=0.005),但与对照组无相关性(r=0.2,P=0.6)。
Fontan 循环青少年肝磁共振弛豫率和剪切波弹性成像值升高提示存在肝纤维化或淤血。中心静脉压与 T1 时间有关。MR 弛豫率和弹性成像检测到的变化不同;因此,在监测肝纤维化时,这两种技术不应互换使用。