Section of Hematology/Oncology and Center for Clinical Cancer Genetics and.
Section of Pulmonary and Critical Care, Department of Medicine, The University of Chicago, Chicago, IL.
Blood Adv. 2020 Oct 13;4(19):4873-4886. doi: 10.1182/bloodadvances.2020001721.
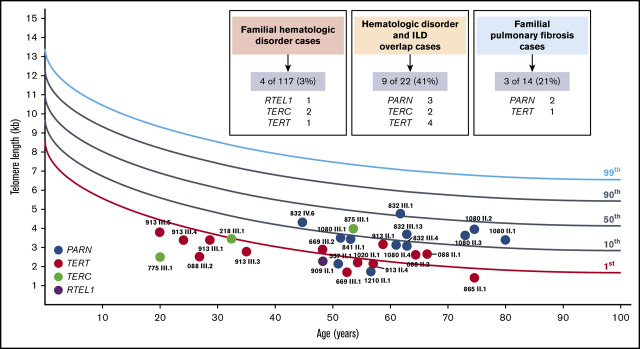
Telomere biology disorders (TBDs) present heterogeneously, ranging from infantile bone marrow failure associated with very short telomeres to adult-onset interstitial lung disease (ILD) with normal telomere length. Yield of genetic testing and phenotypic spectra for TBDs caused by the expanding list of telomere genes in adults remain understudied. Thus, we screened adults aged ≥18 years with a personal and/or family history clustering hematologic disorders and/or ILD enrolled on The University of Chicago Inherited Hematologic Disorders Registry for causative variants in 13 TBD genes. Sixteen (10%) of 153 probands carried causative variants distributed among TERT (n = 6), TERC (n = 4), PARN (n = 5), or RTEL1 (n = 1), of which 19% were copy number variants. The highest yield (9 of 22 [41%]) was in families with mixed hematologic and ILD presentations, suggesting that ILD in hematology populations and hematologic abnormalities in ILD populations warrant TBD genetic testing. Four (3%) of 117 familial hematologic disorder families without ILD carried TBD variants, making TBD second to only DDX41 in frequency for genetic diagnoses in this population. Phenotypes of 17 carriers with heterozygous PARN variants included 4 (24%) with hematologic abnormalities, 67% with lymphocyte telomere lengths measured by flow cytometry and fluorescence in situ hybridization at or above the 10th percentile, and a high penetrance for ILD. Alternative etiologies for cytopenias and/or ILD such as autoimmune features were noted in multiple TBD families, emphasizing the need to maintain clinical suspicion for a TBD despite the presence of alternative explanations.
端粒生物学障碍(TBD)表现多样,从与极短端粒相关的婴儿期骨髓衰竭到成人起病的间质性肺病(ILD)伴正常端粒长度。由于成人端粒基因列表的不断扩大,遗传检测的结果和 TBD 的表型谱对于 TBD 的研究仍然不足。因此,我们筛选了年龄≥18 岁、有个人和/或家族血液系统疾病和/或 ILD 聚集史、参加芝加哥大学遗传性血液疾病登记处的成年人,以寻找 13 个 TBD 基因中的致病变异。在 153 名先证者中,有 16 名(10%)携带致病变异,分布在 TERT(n=6)、TERC(n=4)、PARN(n=5)或 RTEL1(n=1)中,其中 19%为拷贝数变异。最高的检出率(22 个中有 9 个[41%])出现在同时具有血液系统和 ILD 表现的家族中,这表明血液系统人群中的 ILD 和 ILD 人群中的血液学异常都需要进行 TBD 基因检测。在 117 个无 ILD 的家族性血液系统疾病家族中,有 4 个(3%)携带 TBD 变异,在该人群中仅次于 DDX41,是仅次于 DDX41 的遗传诊断频率。携带杂合 PARN 变异的 17 名携带者的表型包括 4 名(24%)血液学异常,67%淋巴细胞端粒长度通过流式细胞术和荧光原位杂交测量处于或高于第 10 百分位数,ILD 高外显率。在多个 TBD 家族中,注意到了血细胞减少症和/或 ILD 的其他病因,如自身免疫特征,这强调了尽管存在其他解释,但仍需要保持对 TBD 的临床怀疑。