Infectious Diseases Service, University Hospital of Lausanne, Lausanne, Switzerland.
Infectious Diseases Service, University Hospital of Lausanne, Lausanne, Switzerland.
J Allergy Clin Immunol. 2021 Jan;147(1):99-106.e4. doi: 10.1016/j.jaci.2020.10.001. Epub 2020 Oct 9.
The coronavirus disease 2019 (COVID-19) pandemic has led to surges of patients presenting to emergency departments (EDs) and potentially overwhelming health systems.
We sought to assess the predictive accuracy of host biomarkers at clinical presentation to the ED for adverse outcome.
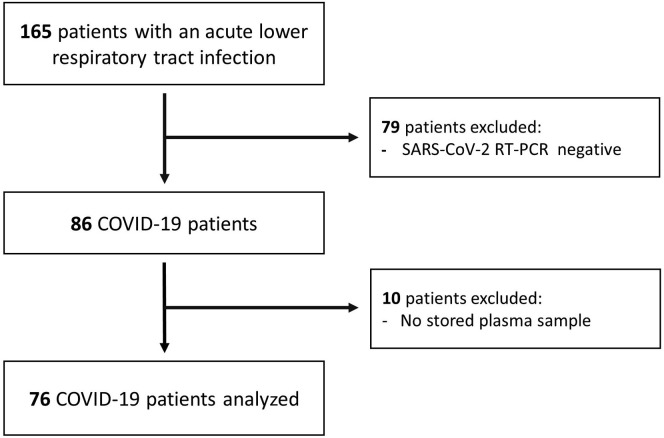
Prospective observational study of PCR-confirmed COVID-19 patients in the ED of a Swiss hospital. Concentrations of inflammatory and endothelial dysfunction biomarkers were determined at clinical presentation. We evaluated the accuracy of clinical signs and these biomarkers in predicting 30-day intubation/mortality, and oxygen requirement by calculating the area under the receiver-operating characteristic curve and by classification and regression tree analysis.
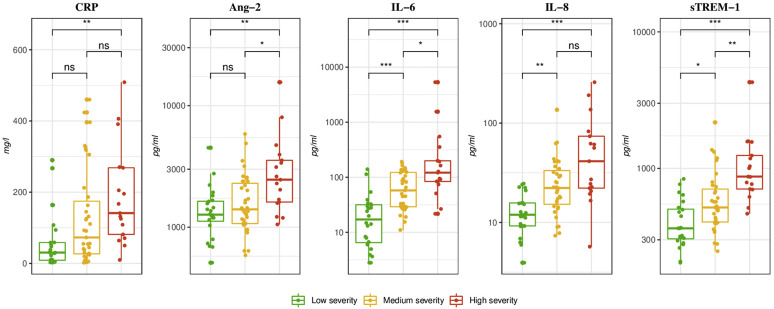
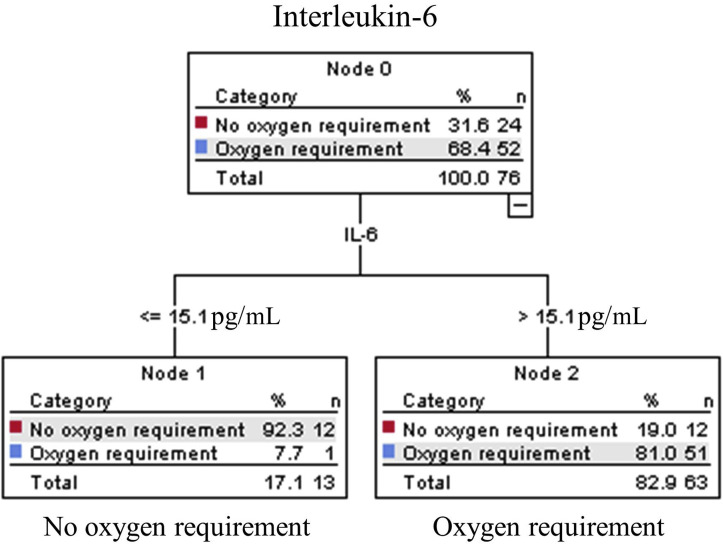
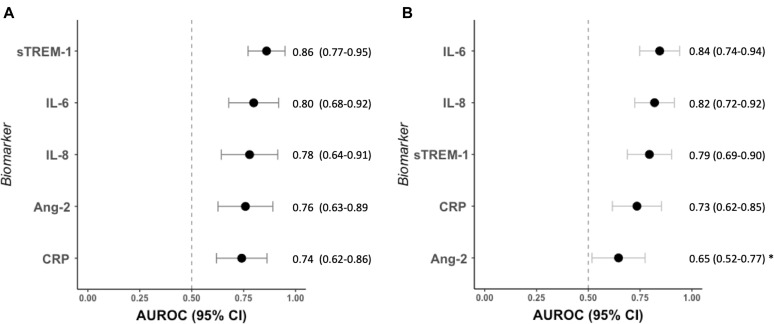
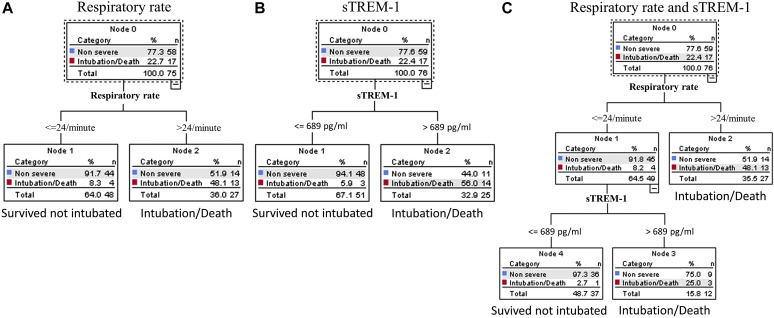
Of 76 included patients with COVID-19, 24 were outpatients or hospitalized without oxygen requirement, 35 hospitalized with oxygen requirement, and 17 intubated/died. We found that soluble triggering receptor expressed on myeloid cells had the best prognostic accuracy for 30-day intubation/mortality (area under the receiver-operating characteristic curve, 0.86; 95% CI, 0.77-0.95) and IL-6 measured at presentation to the ED had the best accuracy for 30-day oxygen requirement (area under the receiver-operating characteristic curve, 0.84; 95% CI, 0.74-0.94). An algorithm based on respiratory rate and sTREM-1 predicted 30-day intubation/mortality with 94% sensitivity and 0.1 negative likelihood ratio. An IL-6-based algorithm had 98% sensitivity and 0.04 negative likelihood ratio for 30-day oxygen requirement.
sTREM-1 and IL-6 concentrations in COVID-19 in the ED have good predictive accuracy for intubation/mortality and oxygen requirement. sTREM-1- and IL-6-based algorithms are highly sensitive to identify patients with adverse outcome and could serve as early triage tools.
2019 年冠状病毒病(COVID-19)大流行导致急诊科(ED)就诊患者激增,可能使卫生系统不堪重负。
我们旨在评估 ED 就诊时宿主生物标志物对不良结局的预测准确性。
这是一项在瑞士医院 ED 进行的 COVID-19 患者的前瞻性观察性研究。在 ED 就诊时测定炎症和内皮功能障碍生物标志物的浓度。我们通过计算受试者工作特征曲线下面积和分类回归树分析,评估临床体征和这些生物标志物预测 30 天插管/死亡率和氧需求的准确性。
在 76 例经 PCR 确诊的 COVID-19 患者中,24 例为门诊或住院且无需吸氧,35 例住院且需要吸氧,17 例插管/死亡。我们发现,髓系细胞表达的可溶性触发受体在预测 30 天插管/死亡率方面具有最佳的预后准确性(受试者工作特征曲线下面积,0.86;95%置信区间,0.77-0.95),而 ED 就诊时测定的白细胞介素 6 对预测 30 天氧需求的准确性最佳(受试者工作特征曲线下面积,0.84;95%置信区间,0.74-0.94)。基于呼吸频率和 sTREM-1 的算法预测 30 天插管/死亡率的敏感性为 94%,阴性似然比为 0.1。基于白细胞介素 6 的算法对 30 天氧需求的敏感性为 98%,阴性似然比为 0.04。
ED 中 COVID-19 患者的 sTREM-1 和白细胞介素 6 浓度对插管/死亡率和氧需求具有良好的预测准确性。基于 sTREM-1 和白细胞介素 6 的算法对识别不良结局患者具有高度敏感性,可作为早期分诊工具。