Department of Respiratory and Critical Care Medicine, the First Affiliated Hospital of Chongqing Medical University, Youyi Road 1, Yuzhong District, Chongqing, 400016, China.
Department of Respiratory and Critical Care Medicine, the People's Hospital of Yubei District, Chongqing, China.
Ther Adv Respir Dis. 2020 Jan-Dec;14:1753466620963019. doi: 10.1177/1753466620963019.
A simple scoring system for triage of suspected patients with COVID-19 is lacking.
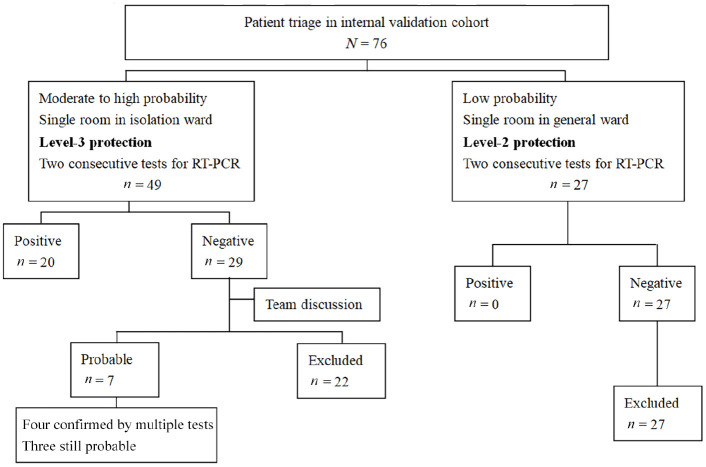
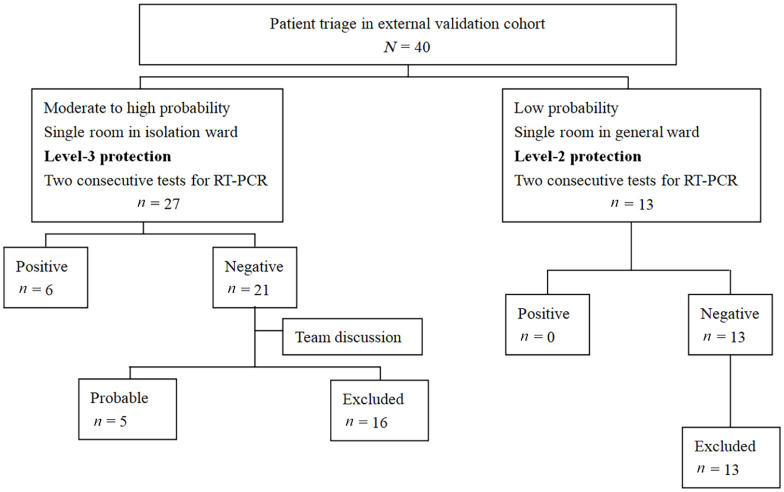
A multi-disciplinary team developed a screening score taking into account epidemiology history, clinical feature, radiographic feature, and routine blood test. At fever clinics, the screening score was used to identify the patients with moderate to high probability of COVID-19 among all the suspected patients. The patients with moderate to high probability of COVID-19 were allocated to a single room in an isolation ward with level-3 protection. And those with low probability were allocated to a single room in a general ward with level-2 protection. At the isolation ward, the screening score was used to identify the confirmed and probable cases after two consecutive real-time reverse transcription polymerase chain reaction (RT-PCR) tests. The data in the People's Hospital of Changshou District were used for internal validation and those in the People's Hospital of Yubei District for external validation.
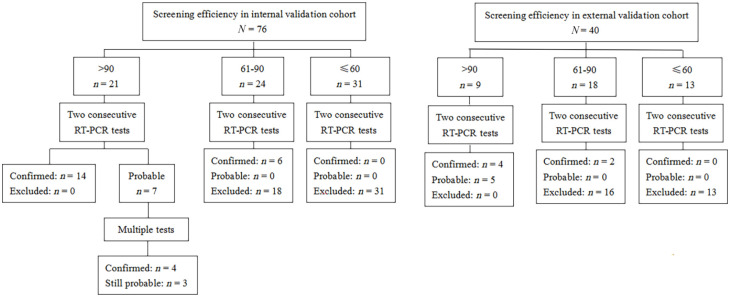
We enrolled 76 and 40 patients for internal and external validation, respectively. In the internal validation cohort, the area under the curve of receiver operating characteristics (AUC) was 0.96 [95% confidence interval (CI): 0.89-0.99] for the diagnosis of moderate to high probability of cases among all the suspected patients. Using 60 as cut-off value, the sensitivity and specificity were 88% and 93%, respectively. In the isolation ward, the AUC was 0.94 (95% CI: 0.83-0.99) for the diagnosis of confirmed and probable cases. Using 90 as cut-off value, the sensitivity and specificity were 78% and 100%, respectively. These results were confirmed in the validation cohort.
The scoring system provides a reference on COVID-19 triage in fever clinics to reduce misdiagnosis and consumption of protective supplies.
目前缺乏一种用于 COVID-19 疑似患者分诊的简便评分系统。
一个多学科团队开发了一种考虑了流行病学史、临床特征、影像学特征和常规血液检查的筛查评分。在发热门诊,使用该评分系统来识别所有疑似患者中具有中度至高度 COVID-19 可能性的患者。将具有中度至高度 COVID-19 可能性的患者分配到隔离病房的单人房间中,并进行 3 级防护。将低度可能性的患者分配到普通病房的单人房间中,并进行 2 级防护。在隔离病房,使用该评分系统在两次连续的实时逆转录聚合酶链反应(RT-PCR)检测后,对确诊和可能病例进行识别。使用长寿区人民医院的数据进行内部验证,使用渝北区人民医院的数据进行外部验证。
我们分别纳入了 76 例和 40 例患者进行内部和外部验证。在内部验证队列中,用于诊断所有疑似患者中具有中度至高度可能性病例的受试者工作特征(ROC)曲线下面积(AUC)为 0.96(95%置信区间:0.89-0.99)。使用 60 作为截断值时,灵敏度和特异性分别为 88%和 93%。在隔离病房中,用于诊断确诊和可能病例的 AUC 为 0.94(95%置信区间:0.83-0.99)。使用 90 作为截断值时,灵敏度和特异性分别为 78%和 100%。这些结果在验证队列中得到了验证。
该评分系统为发热门诊的 COVID-19 分诊提供了参考,以减少误诊和防护用品的消耗。