Department of Emergency Medicine, Yale University School of Medicine, New Haven, CT.
Department of Internal Medicine, Section of Cardiovascular Medicine, Yale University School of Medicine, New Haven, CT; Department of Computer Science, Yale University, New Haven, CT.
Ann Emerg Med. 2020 Oct;76(4):442-453. doi: 10.1016/j.annemergmed.2020.07.022. Epub 2020 Jul 21.
The goal of this study is to create a predictive, interpretable model of early hospital respiratory failure among emergency department (ED) patients admitted with coronavirus disease 2019 (COVID-19).
This was an observational, retrospective, cohort study from a 9-ED health system of admitted adult patients with severe acute respiratory syndrome coronavirus 2 (COVID-19) and an oxygen requirement less than or equal to 6 L/min. We sought to predict respiratory failure within 24 hours of admission as defined by oxygen requirement of greater than 10 L/min by low-flow device, high-flow device, noninvasive or invasive ventilation, or death. Predictive models were compared with the Elixhauser Comorbidity Index, quick Sequential [Sepsis-related] Organ Failure Assessment, and the CURB-65 pneumonia severity score.
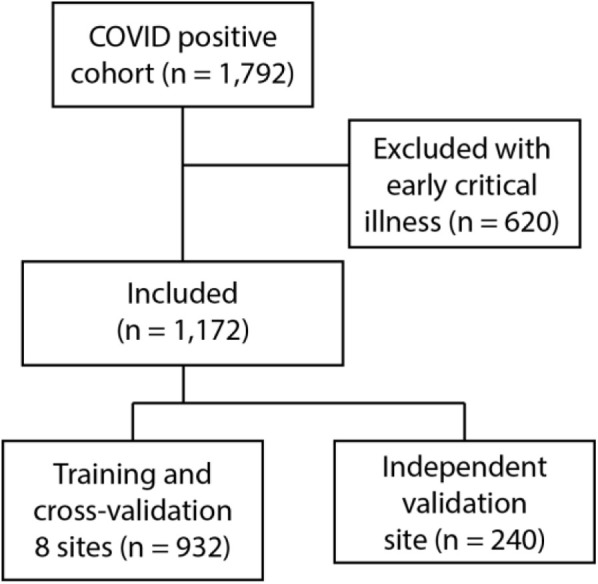
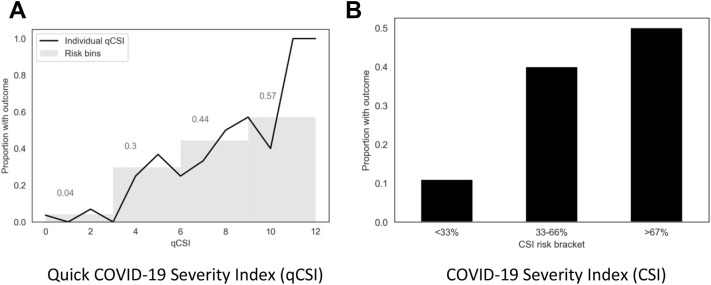
During the study period, from March 1 to April 27, 2020, 1,792 patients were admitted with COVID-19, 620 (35%) of whom had respiratory failure in the ED. Of the remaining 1,172 admitted patients, 144 (12.3%) met the composite endpoint within the first 24 hours of hospitalization. On the independent test cohort, both a novel bedside scoring system, the quick COVID-19 Severity Index (area under receiver operating characteristic curve mean 0.81 [95% confidence interval {CI} 0.73 to 0.89]), and a machine-learning model, the COVID-19 Severity Index (mean 0.76 [95% CI 0.65 to 0.86]), outperformed the Elixhauser mortality index (mean 0.61 [95% CI 0.51 to 0.70]), CURB-65 (0.50 [95% CI 0.40 to 0.60]), and quick Sequential [Sepsis-related] Organ Failure Assessment (0.59 [95% CI 0.50 to 0.68]). A low quick COVID-19 Severity Index score was associated with a less than 5% risk of respiratory decompensation in the validation cohort.
A significant proportion of admitted COVID-19 patients progress to respiratory failure within 24 hours of admission. These events are accurately predicted with bedside respiratory examination findings within a simple scoring system.
本研究的目标是建立一个预测性的、可解释的急诊科(ED)因 2019 年冠状病毒病(COVID-19)入院患者早期院内呼吸衰竭的模型。
这是一项来自一个有 9 个 ED 的健康系统的观察性、回顾性队列研究,纳入的是因严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)和需要氧疗但不超过 6 L/min 的成年患者。我们试图预测入院后 24 小时内需要大于 10 L/min 低流量设备、高流量设备、无创或有创通气或死亡的呼吸衰竭。预测模型与 Elixhauser 合并症指数、快速序贯(Sepsis 相关)器官衰竭评估和 CURB-65 肺炎严重程度评分进行了比较。
在 2020 年 3 月 1 日至 4 月 27 日的研究期间,有 1792 名患者因 COVID-19 入院,其中 620 名(35%)在 ED 出现呼吸衰竭。在其余 1172 名入院患者中,有 144 名(12.3%)在入院后 24 小时内符合复合终点。在独立的测试队列中,一个新的床边评分系统,快速 COVID-19 严重程度指数(ROC 曲线下面积均值为 0.81[95%置信区间{CI}为 0.73 至 0.89])和一个机器学习模型,COVID-19 严重程度指数(均值为 0.76[95%CI 为 0.65 至 0.86])均优于 Elixhauser 死亡率指数(均值为 0.61[95%CI 为 0.51 至 0.70])、CURB-65(0.50[95%CI 为 0.40 至 0.60])和快速序贯(Sepsis 相关)器官衰竭评估(0.59[95%CI 为 0.50 至 0.68])。低快速 COVID-19 严重程度指数评分与验证队列中小于 5%的呼吸失代偿风险相关。
很大一部分因 COVID-19 入院的患者在入院后 24 小时内进展为呼吸衰竭。这些事件可以通过床边呼吸检查结果在一个简单的评分系统中准确预测。