Department of Surgery and Critical Care Medicine, University of Pittsburgh, Pittsburgh, Pennsylvania.
Pittsburgh Trauma Research Center, Pittsburgh, Pennsylvania.
JAMA Netw Open. 2020 Oct 1;3(10):e2016869. doi: 10.1001/jamanetworkopen.2020.16869.
Prehospital plasma administration improves survival in injured patients at risk for hemorrhagic shock and transported by air ambulance. Traumatic brain injury (TBI) is a leading cause of death following trauma, but few early interventions improve outcomes.
To assess the association between prehospital plasma and survival in patients with TBI.
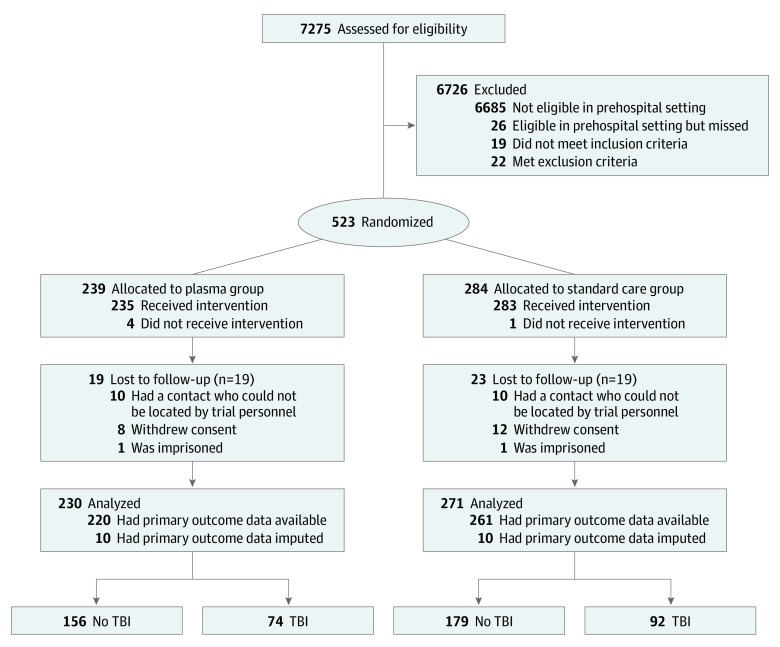
DESIGN, SETTING, AND PARTICIPANTS: The Prehospital Air Medical Plasma (PAMPer) trial was a pragmatic, multicenter, phase 3, cluster randomized clinical trial involving injured patients who were at risk for hemorrhagic shock during air medical transport to a trauma center. The trial was conducted at 6 US sites with 9 level-I trauma centers (comprising 27 helicopter emergency services bases). The original trial analyzed 501 patients, including 230 patients who were randomized to receive plasma and 271 randomized to standard care resuscitation. This secondary analysis of a predefined subgroup included patients with TBI. Data analysis was performed from October 2019 to February 2020.
Patients were randomized to receive standard care fluid resuscitation or 2 units of thawed plasma.
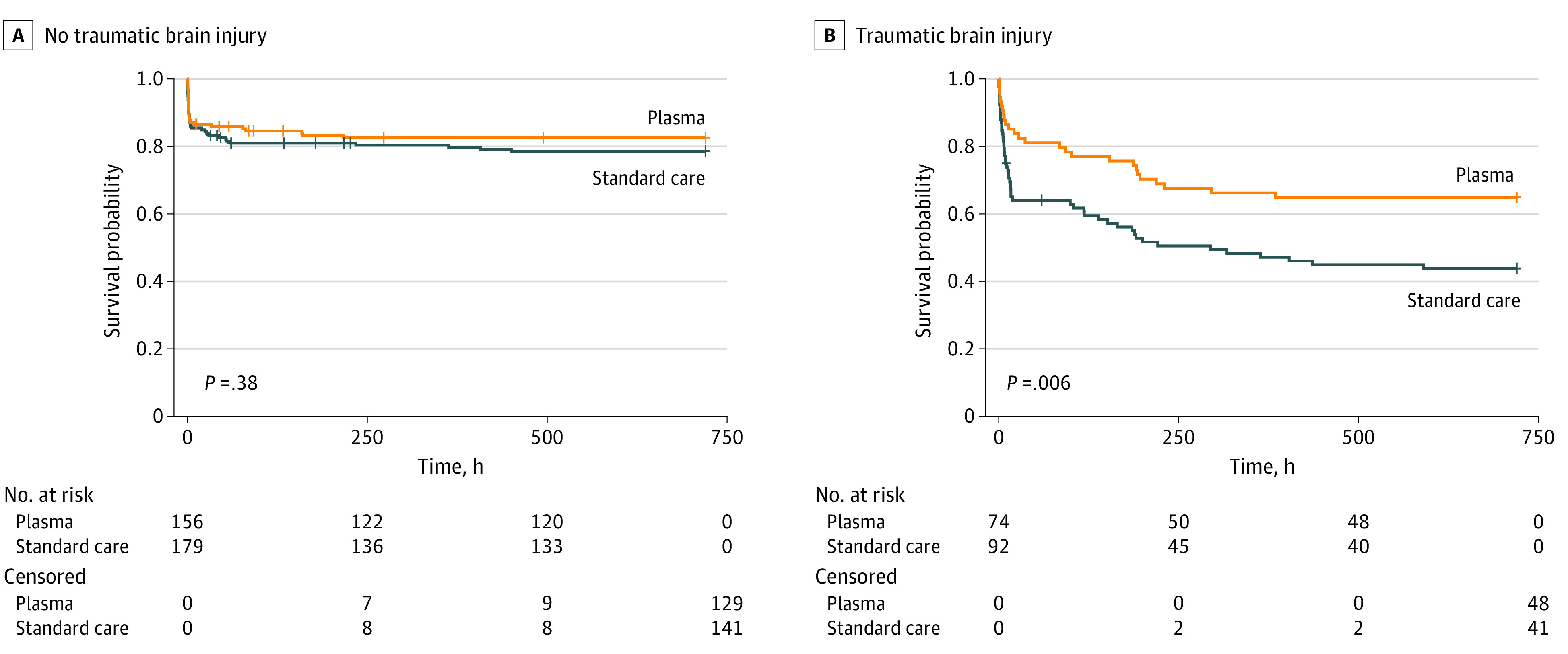
The primary outcome was mortality at 30 days. Patients with TBI were prespecified as a subgroup for secondary analysis and for measurement of markers of brain injury. The 30-day survival benefit of prehospital plasma in subgroups with and without TBI as diagnosed by computed tomography was characterized using Kaplan-Meier survival analysis and Cox proportional hazard regression.
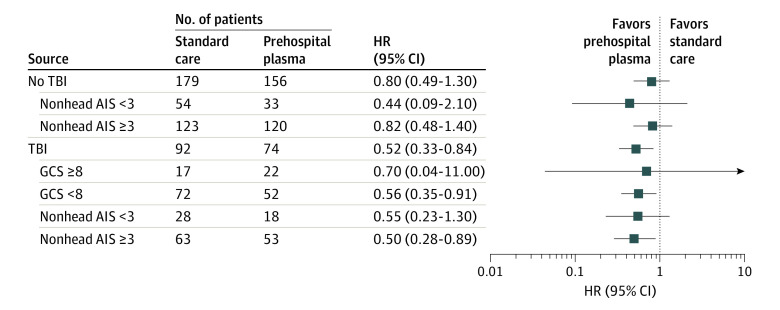
In total, 166 patients had TBI (median [interquartile range] age, 43.00 [25.00-59.75] years; 125 men [75.3%]). When compared with the 92 patients who received standard care, the 74 patients with TBI who received prehospital plasma had improved 30-day survival even after adjustment for multiple confounders and assessment of the degree of brain injury with clinical variables and biomarkers (hazard ratio [HR], 0.55; 95% CI, 0.33-0.94; P = .03). Receipt of prehospital plasma was associated with improved survival among patients with TBI with a prehospital Glasgow Coma Scale score of less than 8 (HR, 0.56; 95% CI, 0.35-0.91) and those with polytrauma (HR, 0.50; 95% CI, 0.28-0.89). Patients with TBI transported from the scene of injury had improved survival following prehospital plasma administration (HR, 0.45; 95% CI, 0.26-0.80; P = .005), whereas patients who were transferred from an outside hospital showed no difference in survival for the plasma intervention (HR, 1.00; 95% CI, 0.33-3.00; P = .99).
These findings are exploratory, but they suggest that receipt of prehospital plasma is associated with improved survival in patients with computed tomography-positive TBI. The prehospital setting may be a critical period to intervene in the care of patients with TBI. Future studies are needed to confirm the clinical benefits of early plasma resuscitation following TBI and concomitant polytrauma.
ClinicalTrials.gov Identifier: NCT01818427.
在因出血性休克有风险并通过空中救护转运的受伤患者中,院前输注血浆可提高生存率。创伤性脑损伤(TBI)是创伤后死亡的主要原因,但很少有早期干预措施能改善预后。
评估院前输注血浆与 TBI 患者生存之间的关联。
设计、地点和参与者:Prehospital Air Medical Plasma(PAMPer)试验是一项实用的、多中心、3 期、集群随机临床试验,涉及有在转运到创伤中心途中发生出血性休克风险的受伤患者。该试验在 6 个美国地点的 9 个一级创伤中心进行(包括 27 个直升机紧急医疗服务基地)。最初的试验分析了 501 名患者,其中 230 名患者被随机分配接受血浆治疗,271 名随机接受标准复苏治疗。本二次分析纳入了 TBI 患者,作为一个预先设定的亚组进行分析。数据分析于 2019 年 10 月至 2020 年 2 月进行。
患者被随机分配接受标准液体复苏或 2 单位解冻血浆。
主要结局为 30 天死亡率。TBI 患者被指定为二次分析和测量脑损伤标志物的亚组。使用 Kaplan-Meier 生存分析和 Cox 比例风险回归,描述亚组中有无 CT 诊断的 TBI 的患者中,院前输注血浆在 30 天的生存获益。
共有 166 名患者患有 TBI(中位数[四分位数范围]年龄,43.00[25.00-59.75]岁;125 名男性[75.3%])。与接受标准护理的 92 名患者相比,74 名 TBI 患者接受了院前血浆治疗,甚至在调整了多种混杂因素后,在评估了临床变量和生物标志物的脑损伤程度后,30 天的生存率仍有所改善(风险比[HR],0.55;95%CI,0.33-0.94;P=0.03)。在院前格拉斯哥昏迷量表评分低于 8 的 TBI 患者(HR,0.56;95%CI,0.35-0.91)和多发伤患者(HR,0.50;95%CI,0.28-0.89)中,接受院前血浆治疗与生存率的提高相关。接受院前血浆治疗的创伤现场转运患者的生存率有所提高(HR,0.45;95%CI,0.26-0.80;P=0.005),而从其他医院转来的患者在血浆干预方面的生存率没有差异(HR,1.00;95%CI,0.33-3.00;P=0.99)。
这些发现是探索性的,但它们表明,院前输注血浆与 CT 阳性 TBI 患者的生存率提高有关。院前阶段可能是干预 TBI 患者治疗的关键时期。需要进一步的研究来证实 TBI 后早期血浆复苏和同时多发伤的临床获益。
ClinicalTrials.gov 标识符:NCT01818427。