Sommerburg Olaf, Hammermann Jutta
Division of Pediatric Pulmonology & Allergy and Cystic Fibrosis Center, Department of Pediatrics III, University of Heidelberg, Im Neuenheimer Feld 430, D-69120 Heidelberg, Germany.
Translational Lung Research Center Heidelberg (TLRC), Member of the German Center for Lung Research (DZL), Im Neuenheimer Feld 350, D-69120 Heidelberg, Germany.
Int J Neonatal Screen. 2020 Mar 30;6(2):28. doi: 10.3390/ijns6020028. eCollection 2020 Jun.
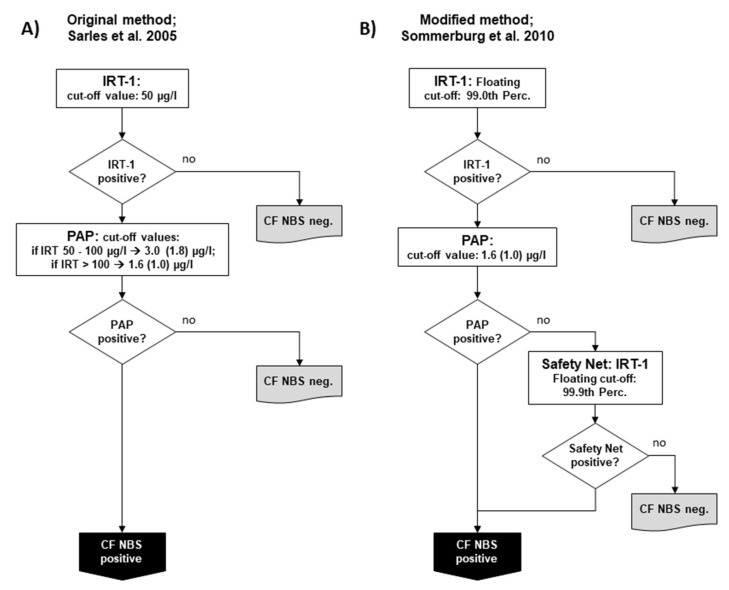
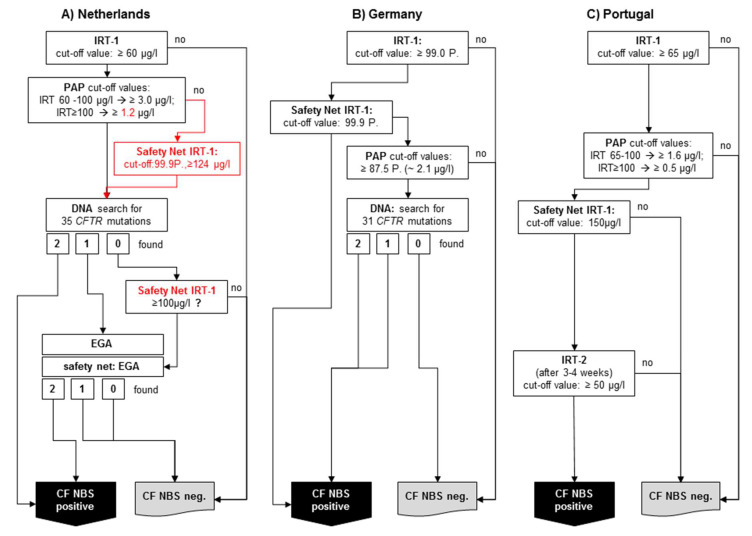
There are currently four countries and one local region in Europe that use PAP in their newborn screening programme. The first country to employ PAP at a national level was the Netherlands, which started using IRT/PAP/DNA/EGA in 2011. Germany followed in 2016 with a slightly different IRT/PAP/DNA strategy. Portugal also started in 2016, but with an IRT/PAP/IRT programme, and in 2017, Austria changed its IRT/IRT protocol to an IRT/PAP/IRT program. In 2018, Catalonia started to use an IRT/PAP/IRT/DNA strategy. The strengths of PAP are the avoidance of carrier detection and a lower detection rate of CFSPID. PAP seems to have advantages in detecting CF in ethnically-diverse populations, as it is a biochemical approach to screening, which looks for pancreatic injury. Compared to an IRT/IRT protocol, an IRT/PAP protocol leads to earlier diagnoses. While PAP can be assessed with the same screening card as the first IRT, the second IRT in an IRT/IRT protocol requires a second heel prick around the 21st day of the patient's life. However, IRT/PAP has two main weaknesses. First, an IRT/PAP protocol seems to have a lower sensitivity compared to a well-functioning IRT/DNA protocol, and second, IRT/PAP that is performed as a purely biochemical protocol has a very low positive predictive value. However, if the advantages of PAP are to be exploited, a combination of IRT/PAP with genetic screening or a second IRT as a third tier could be an alternative for a sufficiently performing CF-NBS protocol.
目前欧洲有四个国家和一个地区在其新生儿筛查项目中使用胰蛋白酶原激活肽(PAP)。在国家层面上首个采用PAP的国家是荷兰,该国于2011年开始使用免疫反应性胰蛋白酶(IRT)/PAP/脱氧核糖核酸(DNA)/扩展基因分型分析(EGA)。德国于2016年跟进,采用了略有不同的IRT/PAP/DNA策略。葡萄牙也于2016年开始,但采用的是IRT/PAP/IRT项目,并且在2017年,奥地利将其IRT/IRT方案改为IRT/PAP/IRT项目。2018年,加泰罗尼亚开始使用IRT/PAP/IRT/DNA策略。PAP的优势在于避免了携带者检测以及先天性脂肪泻样胎粪性肠梗阻(CFSPID)的较低检出率。PAP在检测不同种族人群中的囊性纤维化(CF)方面似乎具有优势,因为它是一种生化筛查方法,旨在寻找胰腺损伤。与IRT/IRT方案相比,IRT/PAP方案能更早做出诊断。虽然PAP可以使用与首次IRT相同的筛查卡进行评估,但IRT/IRT方案中的第二次IRT需要在患者出生后第21天左右再次采集足跟血。然而,IRT/PAP有两个主要缺点。首先,与运行良好的IRT/DNA方案相比,IRT/PAP方案的敏感性似乎较低,其次,作为纯生化方案进行的IRT/PAP的阳性预测值非常低。然而,如果要利用PAP的优势,将IRT/PAP与基因筛查相结合,或者将第二次IRT作为第三层检测,可能是一种用于充分有效的CF新生儿筛查(CF-NBS)方案的替代方法。