University of British Columbia, Vancouver, BC, Canada.
University of Washington/Virginia Mason Medical Center, Seattle, WA, USA.
Arthritis Res Ther. 2020 Oct 19;22(1):247. doi: 10.1186/s13075-020-02335-4.
There has been a shift in recent years to using ultrasound (US) and magnetic resonance imaging (MRI) as first-line investigations for suspected cranial large vessel vasculitis (LVV) and is a new recommendation by the EULAR 2018 guidelines for imaging in LVV. This cross-sectional study compares the performance of US and MRI and contrast-enhanced magnetic resonance angiography (MRA) for detecting vasculitis in patients with giant cell arteritis (GCA).
Patients with new-onset or already diagnosed GCA were recruited. The common temporal arteries and supra-aortic large vessels were evaluated by US and MRI/MRA. Blinded experts read the images and applied a dichotomous score (vasculitis: yes/no) in each vessel.
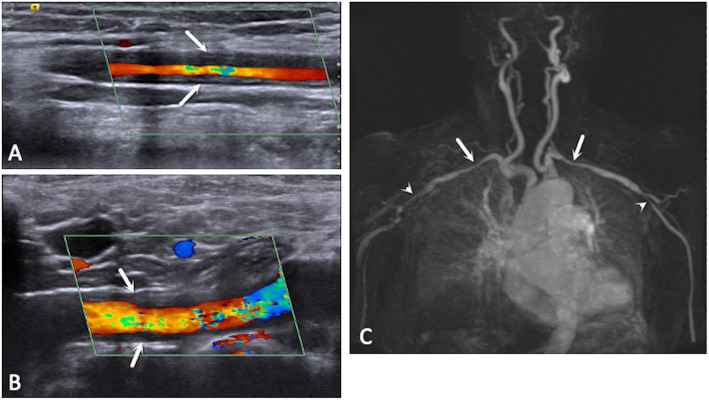
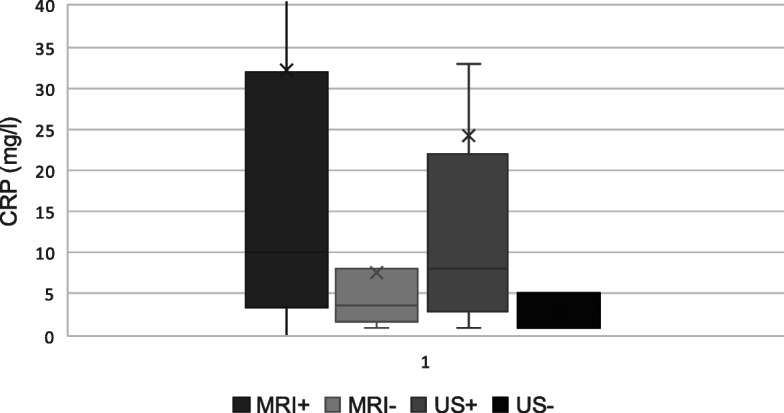
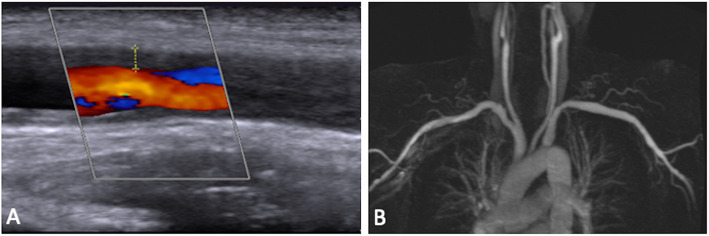
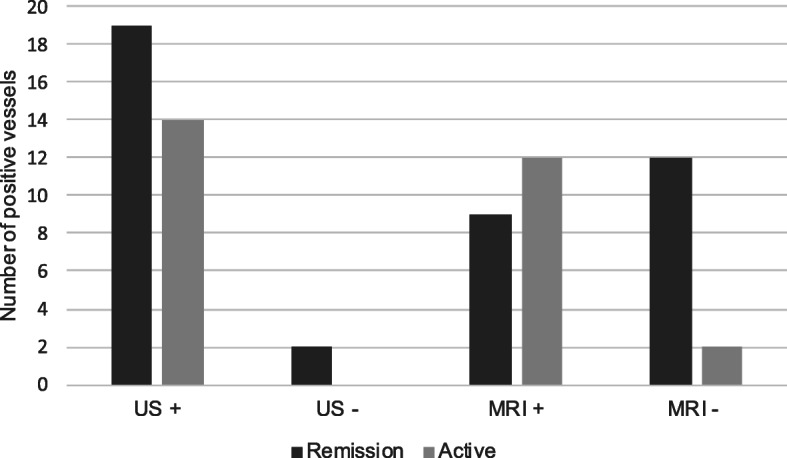
Thirty-seven patients with giant cell arteritis (GCA) were recruited. Two patients were excluded. Of the remaining patients, nine had new-onset disease and 26 had established disease. Mean age was 71 years, and median C-reactive protein (CRP) was 7.5 mg/L. The median time between US and MRI was 1 day. Overall, US revealed vasculitic changes more frequently than MRI (p < 0.001). US detected vascular changes in 37% of vessels compared to 21% with MRI. Among patients with chronic disease, US detected vascular changes in 23% of vessels compared to 7% with MRI in (p < 0.001). The same was true for patients with new-onset disease. US detected vasculitic changes in 22% of vessels and MRI detected disease in 6% (p = 0.0004). Compared to contrast-enhanced MRA, US was more sensitive in detecting vasculitic changes in the large arteries, including the axillary, carotid, and subclavian arteries.
US more frequently detects vasculitic changes in the large arteries compared to contrast-enhanced MRA. When evaluating the cranial vessels, US performs similarly to MRI. This data supports the recommendation that US be considered as a first-line evaluation in patients suspected to have GCA.
近年来,超声(US)和磁共振成像(MRI)已被用于疑似颅大血管血管炎(LVV)的一线检查,这也是 2018 年 EULAR 血管炎成像指南的新推荐。本横断面研究比较了超声和 MRI 及对比增强磁共振血管造影(MRA)在巨细胞动脉炎(GCA)患者中检测血管炎的性能。
招募新诊断或已诊断的 GCA 患者。通过 US 和 MRI/MRA 评估颞动脉和颅外大血管。盲法专家在每支血管上读取图像并应用二分法评分(血管炎:是/否)。
共招募 37 例巨细胞动脉炎(GCA)患者,其中 2 例患者被排除。在其余患者中,9 例为新发疾病,26 例为已确诊疾病。平均年龄为 71 岁,中位 C 反应蛋白(CRP)为 7.5mg/L。US 与 MRI 之间的中位时间为 1 天。总体而言,US 比 MRI 更频繁地显示出血管炎变化(p<0.001)。US 检测到血管变化的血管占 37%,而 MRI 检测到的血管占 21%。在慢性疾病患者中,US 检测到血管变化的血管占 23%,而 MRI 检测到的血管占 7%(p<0.001)。新发病例患者也是如此。US 检测到血管炎变化的血管占 22%,而 MRI 检测到的血管占 6%(p=0.0004)。与对比增强 MRA 相比,US 检测大动脉(包括腋动脉、颈动脉和锁骨下动脉)血管炎变化的敏感性更高。
与对比增强 MRA 相比,US 更频繁地检测到大动脉中的血管炎变化。在评估颅血管时,US 的表现与 MRI 相似。这些数据支持将 US 作为疑似 GCA 患者一线评估的推荐。