Furenäs Eva, Eriksson Peter, Wennerholm Ulla-Britt, Dellborg Mikael
Department of Molecular and Clinical Medicine, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg and Center for Adults with Grown Up Congenital Heart Disease (GUCH), Department of Medicine, Sahlgrenska University Hospital/Östra, Gothenburg, Sweden
Department of Molecular and Clinical Medicine, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg and Center for Adults with Grown Up Congenital Heart Disease (GUCH), Department of Medicine, Sahlgrenska University Hospital/Östra, Gothenburg, Sweden.
Open Heart. 2020 Oct;7(2). doi: 10.1136/openhrt-2020-001293.
To describe the intraindividual changes of heart biomarker levels during and after pregnancy and to evaluate existing cut-off levels for heart failure or myocardial ischaemia in pregnant women.
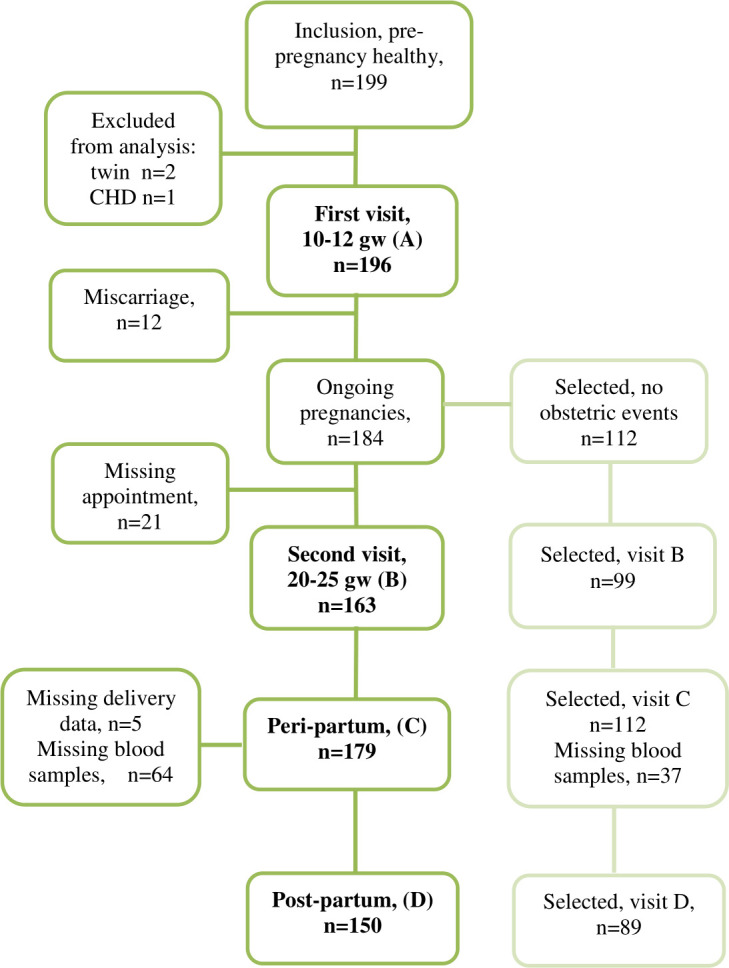
A total of 196 healthy pregnant women were recruited from maternal outpatient clinics and included in the study. Blood samples were obtained on four occasions: at 10-12 gestational weeks (gw), 20-25 gw, after delivery and 6 months postpartum and analysed for N-terminal pro-brain natriuretic peptide (NTproBNP) and high sensitive cardiac troponin T (hs-cTNT). Echocardiography ruled out existing cardiac disease. Estimated glomerular filtration rate (eGFR) was calculated.
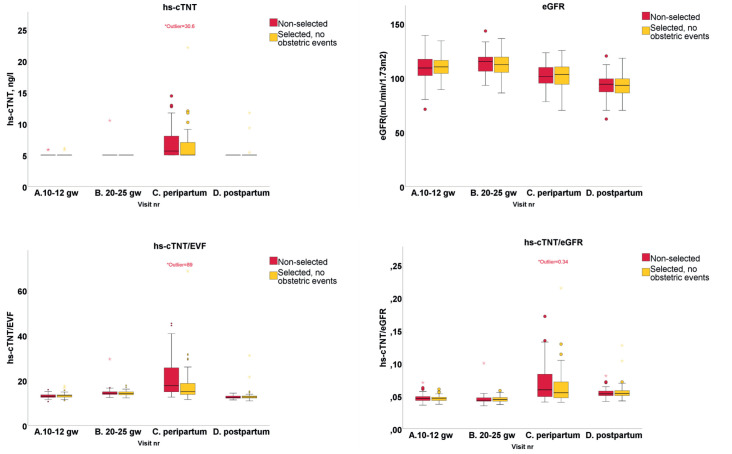
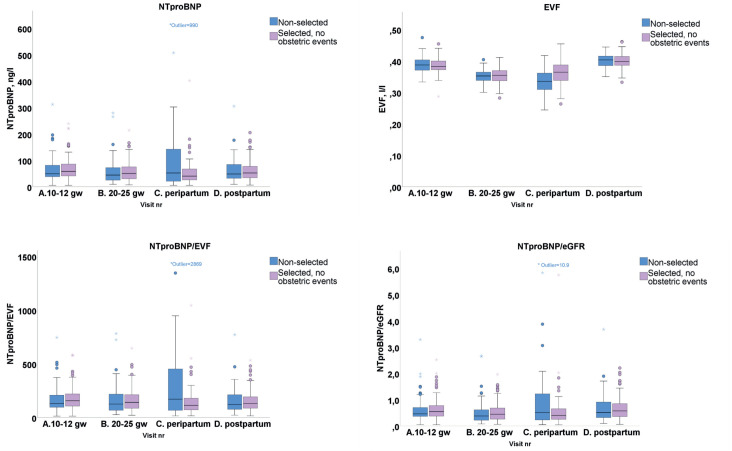
There were significant changes in NTproBNP between the measurements with the highest NTproBNP at 10-12 gw and the lowest value being at 20-25 gw, (with eGFR being the highest). Hs-cTNT was significantly higher at the peripartum measurement compared with the other measurements (p<0.05). Regardless, the 95th percentile for both biomarkers was below cut-off levels of 300 ng/L for NTproBNP and 14 ng/L for hs-cTNT. There was an association between NTproBNP above the upper limit of normal of 125 ng/L and eGFR (p=0.04) and between hs-cTNT >5.0 ng/L and time from delivery to blood sample (p=0.001) at the peripartum measurement. Both were associated with the use of oxytocin.
Existing cut-off values for ruling out heart failure (NTproBNP <300 ng/L) and myocardial ischaemia (hs-cTNT <14 ng/L) are applicable during pregnancy and after delivery. Elevated levels mandate further attention on cardiac symptoms and renal function.
描述孕期及产后心脏生物标志物水平的个体内变化,并评估孕妇心力衰竭或心肌缺血的现有截断值。
从产科门诊招募了196名健康孕妇纳入研究。在四个时间点采集血样:妊娠10 - 12周(gw)、20 - 25 gw、分娩后及产后6个月,检测N末端脑钠肽前体(NTproBNP)和高敏心肌肌钙蛋白T(hs-cTNT)。超声心动图排除现有心脏疾病。计算估计肾小球滤过率(eGFR)。
NTproBNP在各次测量中有显著变化,妊娠10 - 12 gw时NTproBNP最高,20 - 25 gw时最低(此时eGFR最高)。围产期测量时hs-cTNT显著高于其他测量值(p<0.05)。尽管如此,两种生物标志物的第95百分位数均低于NTproBNP的截断值300 ng/L和hs-cTNT的截断值14 ng/L。围产期测量时,NTproBNP高于正常上限125 ng/L与eGFR相关(p = 0.04),hs-cTNT>5.0 ng/L与分娩至血样采集时间相关(p = 0.001)。两者均与缩宫素的使用有关。
排除心力衰竭(NTproBNP<300 ng/L)和心肌缺血(hs-cTNT<14 ng/L)的现有截断值在孕期和产后适用。水平升高时需进一步关注心脏症状和肾功能。