Yeargin Susan, Hirschhorn Rebecca, Grundstein Andrew
Department of Exercise Science, University of South Carolina, Columbia, SC 29208, USA.
School of Kinesiology, Auburn University, Auburn, AL 36849, USA.
Medicina (Kaunas). 2020 Oct 17;56(10):543. doi: 10.3390/medicina56100543.
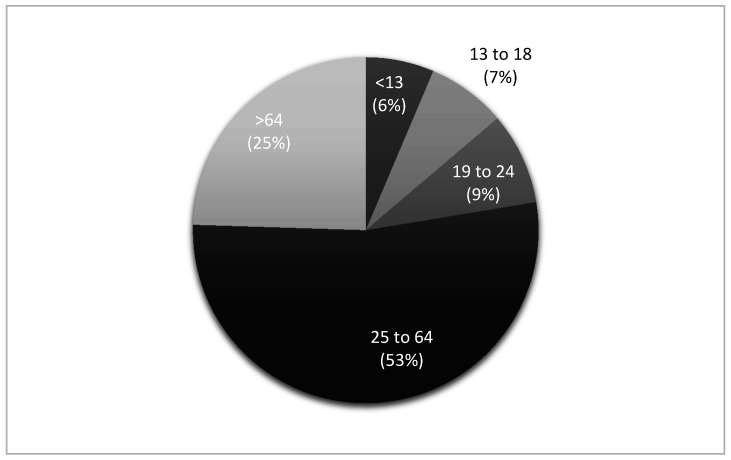
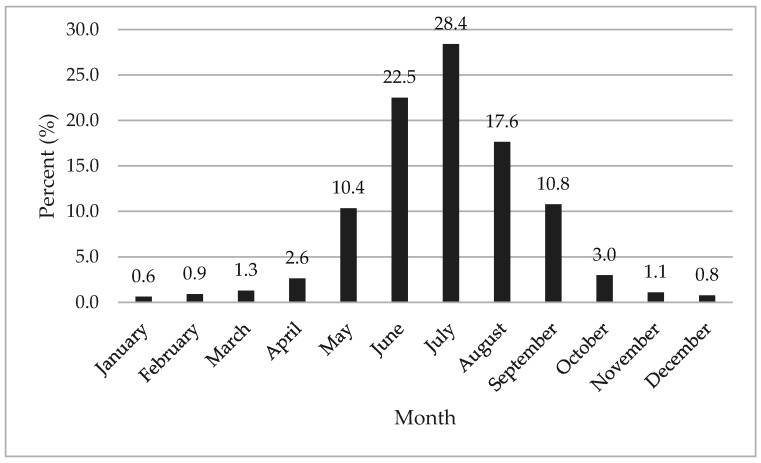
Heat-related illness (HRI) can have significant morbidity and mortality consequences. Research has predominately focused on HRI in the emergency department, yet health care leading up to hospital arrival can impact patient outcomes. Therefore, the purpose of this study was to describe HRI in the prehospital setting. A descriptive epidemiological design was utilized using data from the National Emergency Medical Services (EMS) Information System for the 2017-2018 calendar years. Variables of interest in this study were: patient demographics (age, gender, race), US census division, urbanicity, dispatch timestamp, incident disposition, primary provider impression, and regional temperatures. There were 34,814 HRIs reported. The majority of patients were white ( = 10,878, 55.6%), males ( = 21,818, 62.7%), and in the 25 to 64 age group ( = 18,489, 53.1%). Most HRIs occurred in the South Atlantic US census division ( = 11,732, 33.7%), during the summer ( = 23,873, 68.6%), and in urban areas ( = 27,541, 83.5%). The hottest regions were East South Central, West South Central, and South Atlantic, with peak summer temperatures in excess of 30.0 °C. In the spring and summer, most regions had near normal temperatures within 0.5 °C of the long-term mean. EMS dispatch was called for an HRI predominately between the hours of 11:00 a.m.-6:59 p.m. ( = 26,344, 75.7%), with the majority (27,601, 79.3%) of HRIs considered heat exhaustion and requiring the patient to be treated and transported ( = 24,531, 70.5%). All age groups experienced HRI but particularly those 25 to 64 years old. Targeted education to increase public awareness of HRI in this age group may be needed. Region temperature most likely explains why certain divisions of the US have higher HRI frequency. Afternoons in the summer are when EMS agencies should be prepared for HRI activations. EMS units in high HRI frequency US divisions may need to carry additional treatment interventions for all HRI types.
与热相关的疾病(HRI)可能会导致严重的发病和死亡后果。研究主要集中在急诊科的HRI,但在患者入院前的医疗护理也会影响患者的治疗结果。因此,本研究的目的是描述院前环境中的HRI。采用描述性流行病学设计,使用2017 - 2018历年美国国家紧急医疗服务(EMS)信息系统的数据。本研究感兴趣的变量包括:患者人口统计学特征(年龄、性别、种族)、美国人口普查分区、城市化程度、调度时间戳、事件处置情况、主要提供者的印象以及区域温度。共报告了34,814例HRI。大多数患者为白人(n = 10,878,55.6%),男性(n = 21,818,62.7%),年龄在25至64岁之间(n = 18,489,53.1%)。大多数HRI发生在美国人口普查分区的南大西洋地区(n = 11,732,33.7%),在夏季(n = 23,873,68.6%),以及城市地区(n = 27,541,83.5%)。最热的地区是东中南部、西中南部和南大西洋地区,夏季最高气温超过30.0℃。在春季和夏季,大多数地区的气温接近长期平均气温,偏差在0.5℃以内。EMS调度主要是在上午11:00至下午6:59之间接到HRI报警(n = 26,344,75.7%),大多数(27,601,79.3%)HRI被认为是热衰竭,需要对患者进行治疗并转运(n = 24,531,70.5%)。所有年龄组都有HRI发生,但25至64岁的人群尤为突出。可能需要针对该年龄组开展有针对性的教育,以提高公众对HRI的认识。区域温度很可能解释了为什么美国某些地区的HRI发生率较高。夏季的下午是EMS机构应做好应对HRI准备的时候。美国HRI发生率高的分区的EMS单位可能需要为所有类型的HRI携带额外的治疗干预措施。