Medical University Department, Division of General Internal and Emergency Medicine, Kantonsspital Aarau, Aarau, Switzerland; Medical Faculty of the University of Basel, Switzerland.
Medical University Department, Division of General Internal and Emergency Medicine, Kantonsspital Aarau, Aarau, Switzerland.
Clin Nutr. 2021 Apr;40(4):1843-1850. doi: 10.1016/j.clnu.2020.10.009. Epub 2020 Oct 10.
In polymorbid patients with bronchopulmonary infection, malnutrition is an independent risk factor for mortality. There is a lack of interventional data investigating whether providing nutritional support during the hospital stay in patients at risk for malnutrition presenting with lower respiratory tract infection lowers mortality.
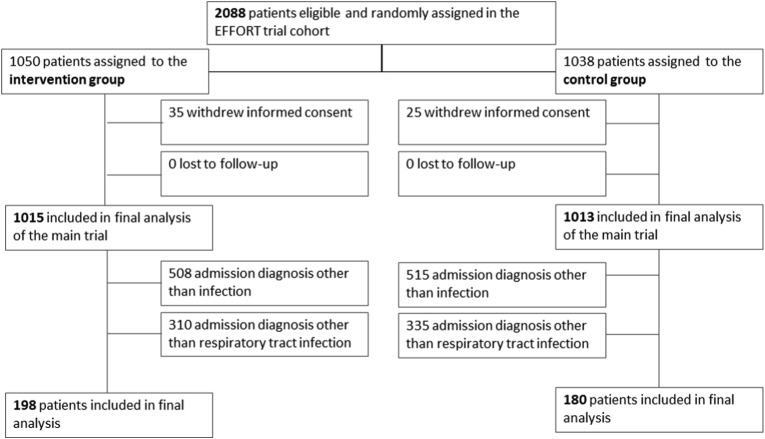
For this secondary analysis of a randomized clinical trial (EFFORT), we analyzed data of a subgroup of patients with confirmed lower respiratory tract infection from an initial cohort of 2028 patients. Patients at nutritional risk (Nutritional Risk Screening [NRS] score ≥3 points) were randomized to receive protocol-guided individualized nutritional support to reach protein and energy goals (intervention group) or standard hospital food (control group). The primary endpoint of this analysis was all-cause 30-day mortality.
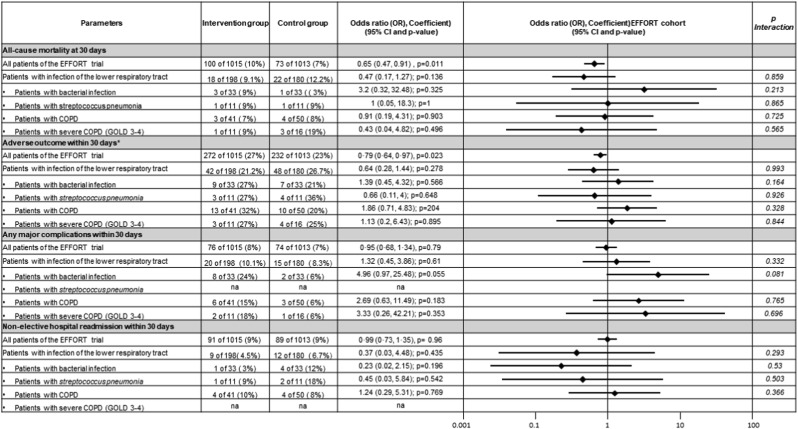
We included 378 of 2028 EFFORT patients (mean age 74.4 years, 24% with COPD) into this analysis. Compared to usual care hospital nutrition, individualized nutritional support to reach caloric and protein goals showed a similar beneficial effect of on the risk of mortality in the subgroup of respiratory tract infection patients as compared to the main EFFORT trial (odds ratio 0.47 [95%CI 0.17 to 1.27, p = 0.136] vs 0.65 [95%CI 0.47 to 0.91, p = 0.011]) with no evidence of a subgroup effect (p for interaction 0.859). Effects were also similar among different subgroups based on etiology and type of respiratory tract infection and for other secondary endpoints.
This subgroup analysis from a large nutrition support trial suggests that patients at nutritional risk as assessed by NRS 2002 presenting with bronchopulmonary infection to the hospital likely have a mortality benefit from individualized inhospital nutritional support. The small sample size and limited statistical power calls for larger nutritional studies focusing on this highly vulnerable patient population.
Registered under ClinicalTrials.gov Identifier no. NCT02517476.
在患有肺部感染的多种合并症的患者中,营养不良是死亡的独立危险因素。缺乏干预性数据表明,对于存在营养不良风险且患有下呼吸道感染的住院患者,在住院期间提供营养支持是否可以降低死亡率。
本研究为一项随机临床试验(EFFORT)的二次分析,我们分析了来自 2028 例患者初始队列中确诊为下呼吸道感染患者亚组的数据。有营养风险的患者(营养风险筛查 [NRS]评分≥3 分)被随机分为两组:一组接受基于方案的个体化营养支持以达到蛋白质和能量目标(干预组),另一组接受标准医院饮食(对照组)。本分析的主要终点是全因 30 天死亡率。
我们将 2028 例 EFFORT 患者中的 378 例(平均年龄 74.4 岁,24%患有 COPD)纳入本分析。与常规医院营养治疗相比,个体化营养支持以达到热量和蛋白质目标,与 EFFORT 主要试验相比,在呼吸道感染患者亚组中,对死亡率的影响具有相似的有益作用(比值比 0.47 [95%CI 0.17 至 1.27,p=0.136] 与 0.65 [95%CI 0.47 至 0.91,p=0.011]),且无亚组效应的证据(p 交互作用=0.859)。根据病因和呼吸道感染类型以及其他次要终点,在不同亚组中,结果也相似。
这项来自大型营养支持试验的亚组分析表明,根据 NRS 2002 评估存在营养风险且因肺部感染入院的患者,可能会从住院期间的个体化营养支持中获益,降低死亡率。但由于样本量小且统计效力有限,因此需要开展更多关注这一高危患者人群的营养研究。
ClinicalTrials.gov 标识符:NCT02517476。