Deaprtment of Pharmacology and Clinical Pharmacy, School of Pharmacy, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia.
Department of Clinical Pharmacy, School of Pharmacy, Institute of Health, Jimma University, Jimma, Ethiopia.
Can Respir J. 2020 Oct 13;2020:4312519. doi: 10.1155/2020/4312519. eCollection 2020.
The pandemic of coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) resulted in an unprecedented public health challenge worldwide. Despite urgent and extensive global efforts, the existing evidence is inconclusive regarding the medications used for the treatment of COVID-19.
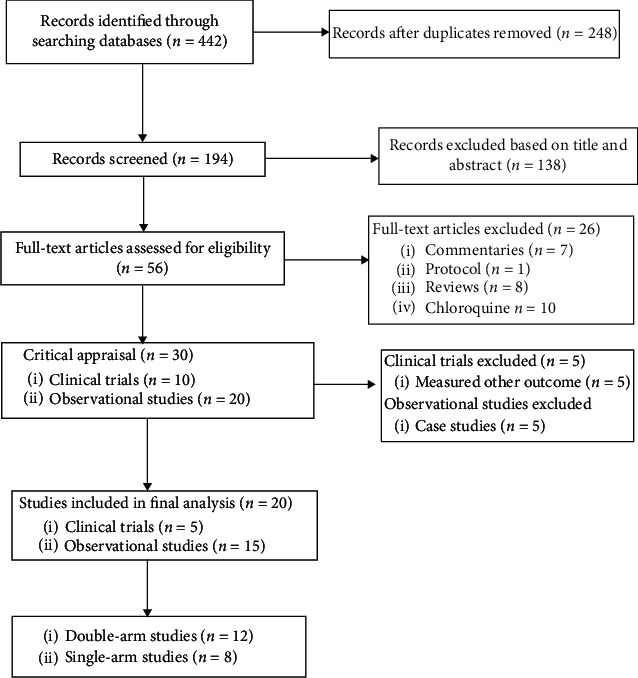
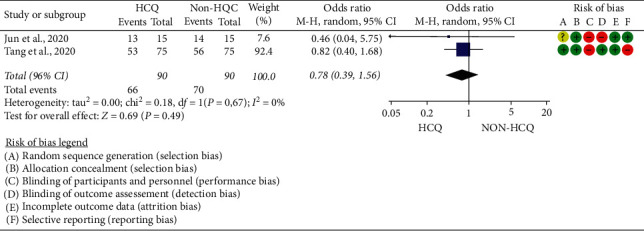
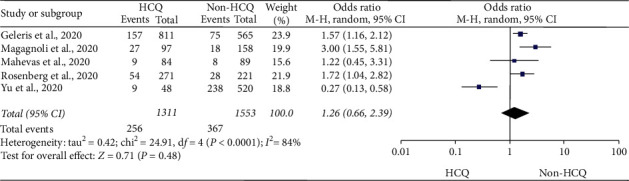
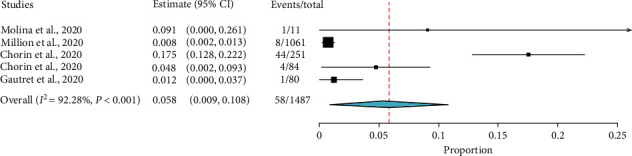
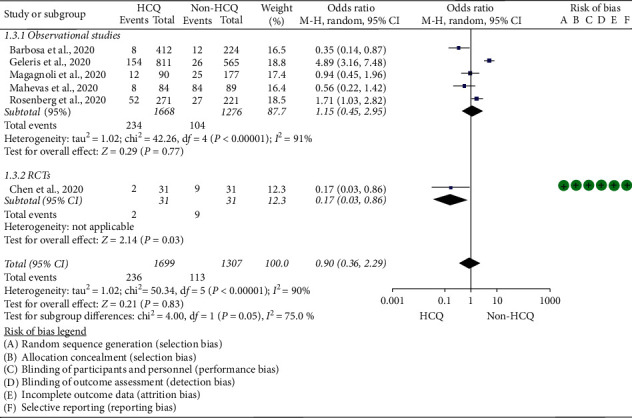
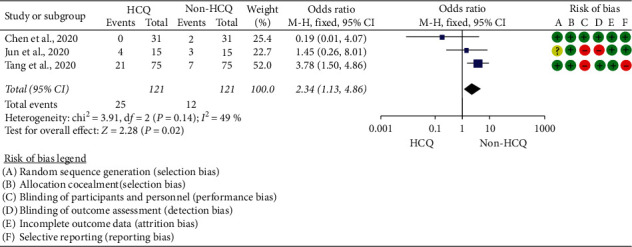
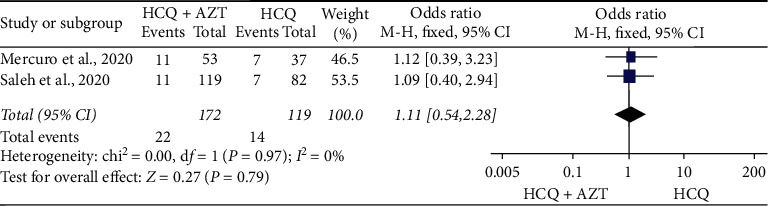
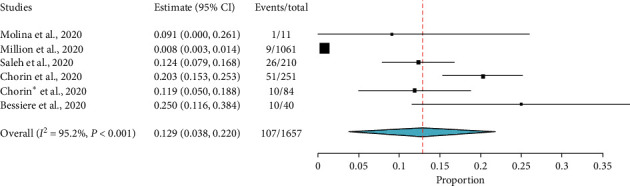
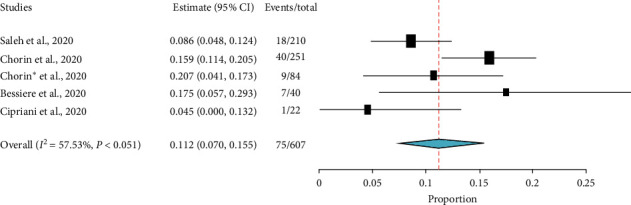
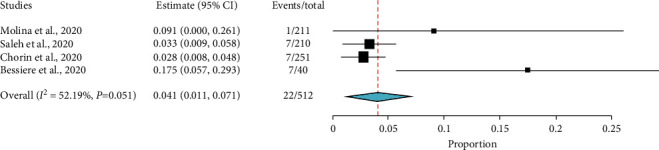
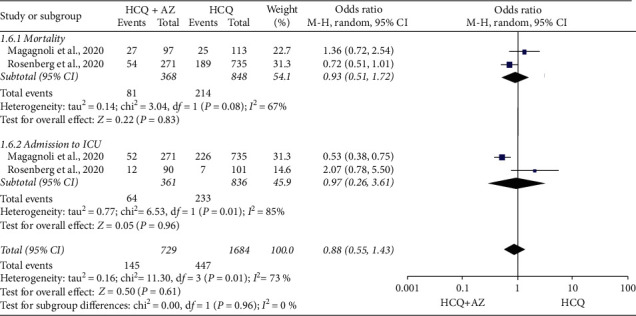
To generate an up-to-date evidence for the clinical safety and efficacy of hydroxychloroquine (HCQ) with or without azithromycin (AZ) among patients treated for COVID-19. . PubMed, Cochrane CENTRAL, LITCOVID, Web of Science, SCOPUS, BioRxiv, Embase, MedRxiv, and Wiley online library were searched from 2019/12/30 to 2020/05/23. . Three investigators assessed the quality of the studies. . Data about study characteristics, effect estimates, and the quality of the studies were extracted by two independent reviewers and cross-checked by the third reviewer. . The data of 6,782 (HCQ group, 3623; HCQ + AZ group, 1,020; control group, 2139) participants were included. HCQ was compared with standard care for virologic efficacy, disease progression, mortality, and adverse effects. HCQ was also compared with HCQ + AZ for QTc prolongation, admission to the intensive care unit, and mortality. The study found HCQ did not alter the rate of virologic cure (OR = 0.78; 95% CI: 0.39-1.56) and the risk of mortality (OR = 1.26; 95% CI: 0.66-2.39). The pooled prevalence for mortality was 5.8% (95% CI: 0.9%-10.8%). Moreover, HCQ did not impact disease progression (OR = 0.9; 95% CI: 0.36-2.29) but resulted in a higher risk of adverse effects (OR = 2.35; 95% CI: 1.15-4.8). HCQ was also compared against HCQ + AZ, and no difference was observed in QTc prolongation above 500 ms (OR = 1.11; 95% CI: 0.54-2.28), admission to the intensive care unit (OR = 0.92; 95% CI: 0.52-1.63), and mortality (OR = 0.88; 95% CI: 0.55-1.43). However, in the analysis of single-arm studies, about 11.2% (95% CI: 7.0%-15.5%) of patients have developed an absolute increase of QTc greater than 500 ms, and 4.1% (95% CI: 1.1%-7.1%) of patients discontinued their medication.
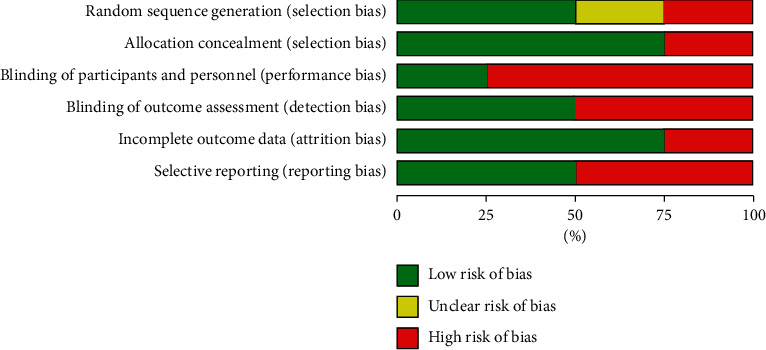
This meta-analysis and systematic review, which included a limited number of poorly designed studies of patients with COVID-19, revealed HCQ is intolerable, unsafe, and not efficacious. Similarly, HCQ + AZ combination was not different from HCQ alone in curbing mortality and ICU admission.
由严重急性呼吸系统综合征冠状病毒 2(SARS-CoV-2)引起的 2019 年冠状病毒病(COVID-19)大流行在全球范围内造成了前所未有的公共卫生挑战。尽管全球紧急和广泛地努力,但是对于 COVID-19 的治疗药物,现有证据尚无定论。
生成羟氯喹(HCQ)单独或联合阿奇霉素(AZ)治疗 COVID-19 患者的临床安全性和疗效的最新证据。
从 2019 年 12 月 30 日至 2020 年 5 月 23 日,在 PubMed、Cochrane 中央、LITCOVID、Web of Science、SCOPUS、BioRxiv、Embase、MedRxiv 和 Wiley 在线图书馆中进行了检索。
研究设计为前瞻性或回顾性队列研究或病例对照研究,患者在确诊 COVID-19 后接受 HCQ 或 HCQ+AZ 治疗。
研究设计为随机对照试验、病例报告、综述或meta 分析。
由两位独立的研究者筛选文献并提取数据,如有分歧,由第三位研究者进行仲裁。
主要结局指标为病毒学缓解率、疾病进展、死亡率和不良事件发生率。
次要结局指标为 QTc 延长、入住重症监护病房(ICU)和药物停药率。
使用固定效应模型或随机效应模型进行 meta 分析,根据异质性检验结果选择合适的模型。
共纳入 6782 名患者(HCQ 组 3623 名,HCQ+AZ 组 1020 名,对照组 2139 名)。与标准治疗相比,HCQ 并未改善病毒学缓解率(OR=0.78,95%CI:0.39-1.56)或死亡率(OR=1.26,95%CI:0.66-2.39)。HCQ 组的死亡率为 5.8%(95%CI:0.9%-10.8%)。此外,HCQ 并未改善疾病进展(OR=0.9,95%CI:0.36-2.29),但增加了不良事件的风险(OR=2.35,95%CI:1.15-4.8)。与 HCQ+AZ 相比,HCQ 并未导致 QTc 延长超过 500ms(OR=1.11,95%CI:0.54-2.28)、入住 ICU(OR=0.92,95%CI:0.52-1.63)或死亡率(OR=0.88,95%CI:0.55-1.43)的差异。然而,在单臂研究的分析中,约有 11.2%(95%CI:7.0%-15.5%)的患者出现了 QTc 绝对增加超过 500ms,4.1%(95%CI:1.1%-7.1%)的患者停药。
本 meta 分析和系统评价纳入了数量有限的设计不佳的 COVID-19 患者研究,结果显示 HCQ 不耐受、不安全且无效。同样,HCQ+AZ 联合治疗与 HCQ 单独治疗相比,在抑制死亡率和 ICU 入院方面没有差异。