Wu Wenhan, Liu Jianbo, Zhou Zongguang
Institute of Digestive Surgery of Sichuan University, and Department of Gastrointestinal Surgery, West China Hospital, West China School of Medicine, Sichuan University, 610041 Chengdu, Sichuan, China.
Emerg Med Int. 2020 Oct 5;2020:1382475. doi: 10.1155/2020/1382475. eCollection 2020.
Our objective was to comprehensively present the evidence of preoperative risk factors for short-term postoperative mortality of acute mesenteric ischemia after laparotomy.
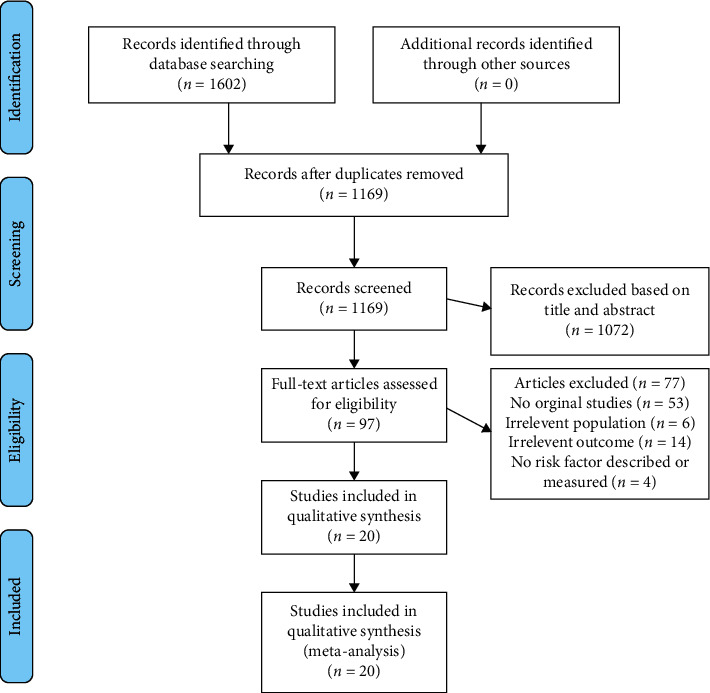
PubMed, Embase, and Google Scholar were searched from January 2000 to January 2020. Studies evaluating the postoperative risk factors for short-term postoperative mortality of acute mesenteric ischemia after laparotomy were included. The outcome extracted were patients' demographics, medical history, and preoperative laboratory tests.
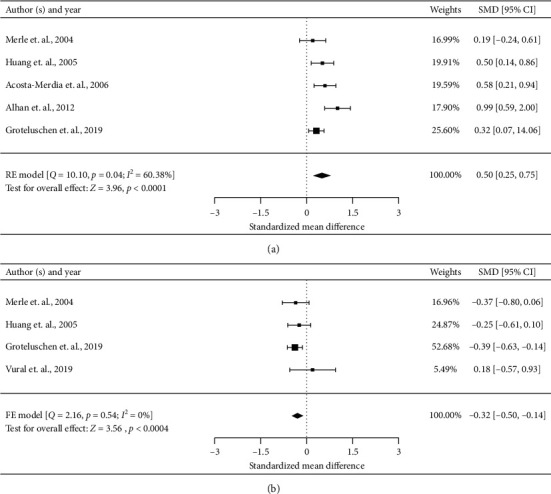
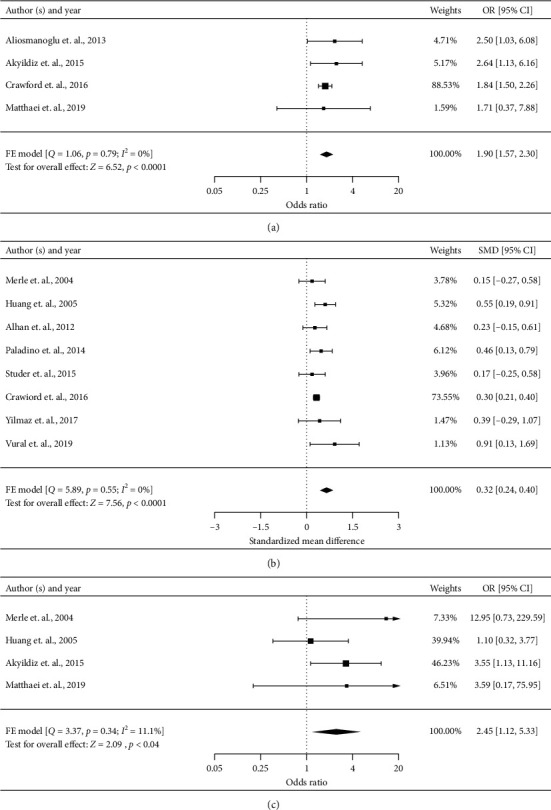
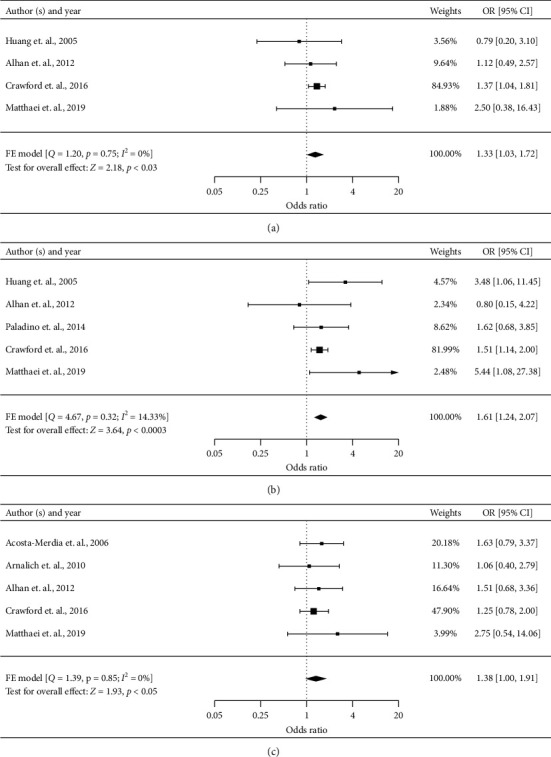
Twenty studies (5011 patients) met the inclusion criteria. Studies were of high quality, with a median Newcastle-Ottawa Scale Score of 7. Summary short-term postoperative mortality was 44.38% (range, 18.80%-67.80%). Across included studies, 49 potential risk factors were examined, at least two studies. Meta-analysis of predictors based on more than three studies identified the following preoperative risk factors for higher short-term postoperative mortality risk: old age (odds ratio [OR], 1.90, 95% confidence interval [CI], 1.57-2.30), arterial occlusive mesenteric ischemia versus mesenteric venous thrombosis (OR, 2.45, 95% CI 1.12-5.33), heart failure (OR 1.33, 95% CI 1.03-1.72), renal disorders (OR 1.61, 95% CI 1.24-2.07), and peripheral vascular disease (OR 1.38, 95% CI 1.00-1.91). Nonsurvivors were older (standardized mean difference [SMD], 0.32, 95% CI 0.24-0.40), had higher creatinine levels (SMD 0.50, 95% CI 0.25-0.75), and had lower platelet counts (SMD -0.32, 95% CI -0.50 to -0.14).
The short-term postoperative mortality of acute mesenteric ischemia who underwent laparotomy is still high. A better understanding of these risk factors may help in the early identification of high-risk patients, optimization of surgical procedure, and improvement of perioperative management.
我们的目的是全面呈现剖腹术后急性肠系膜缺血短期术后死亡率的术前危险因素证据。
检索了2000年1月至2020年1月期间的PubMed、Embase和谷歌学术。纳入评估剖腹术后急性肠系膜缺血短期术后死亡率危险因素的研究。提取的结果包括患者的人口统计学、病史和术前实验室检查。
20项研究(5011例患者)符合纳入标准。研究质量较高,纽卡斯尔-渥太华量表评分中位数为7分。短期术后总体死亡率为44.38%(范围为18.80%-67.80%)。在纳入的研究中,至少两项研究对49个潜在危险因素进行了检查。基于三项以上研究的预测因素的荟萃分析确定了以下术后短期死亡率较高的术前危险因素:老年(比值比[OR],1.90,95%置信区间[CI],1.57-2.30)、动脉闭塞性肠系膜缺血与肠系膜静脉血栓形成(OR,2.45,95%CI 1.12-5.33)、心力衰竭(OR 1.33,95%CI 1.03-1.72)、肾脏疾病(OR 1.61,95%CI 1.24-2.07)和外周血管疾病(OR 1.38,95%CI 1.00-1.91)。非幸存者年龄更大(标准化均数差[SMD],0.32,95%CI 0.24-)。