Burr Adam R, Robins Henry Ian, Bayliss Robert Adam, Baschnagel Andrew M, Welsh James S, Tomé Wolfgang A, Howard Steven P
Department of Human Oncology, University of Wisconsin School of Medicine and Public Health, Carbone Cancer Center, Madison, Wisconsin.
Department of Radiation Oncology, Loyola University Stritch School of Medicine, Chicago, Illinois.
Adv Radiat Oncol. 2020 Jul 8;5(5):834-839. doi: 10.1016/j.adro.2020.06.021. eCollection 2020 Sep-Oct.
Recurrent intracranial metastases after whole-brain irradiation pose a clinical challenge owing to the escalating morbidity associated with their treatment. Although stereotactic radiosurgery is increasingly being used, there are still situations in which whole-brain reirradiation (ReRT) continues to be appropriate. Here, we report our experience using whole-brain pulsed reduced dose rate radiation therapy (PRDR), a method that delivers radiation at a slower rate of 0.067 Gy/min to potentially increase sublethal damage repair and decrease toxicity.
Patients undergoing whole-brain ReRT with PRDR from January 1, 2001 to March 2019 were analyzed. The median PRDR ReRT dose was 26 Gy in 2 Gy fractions, resulting in a median total whole-brain dose of 59.5 Gy. Cox regression analysis was used for multivariate analysis. The Kaplan-Meier method was used for overall survival, progression free survival, and to evaluate the ReRT score. Binary logistic regression was employed to evaluate variables associated with rapid death.
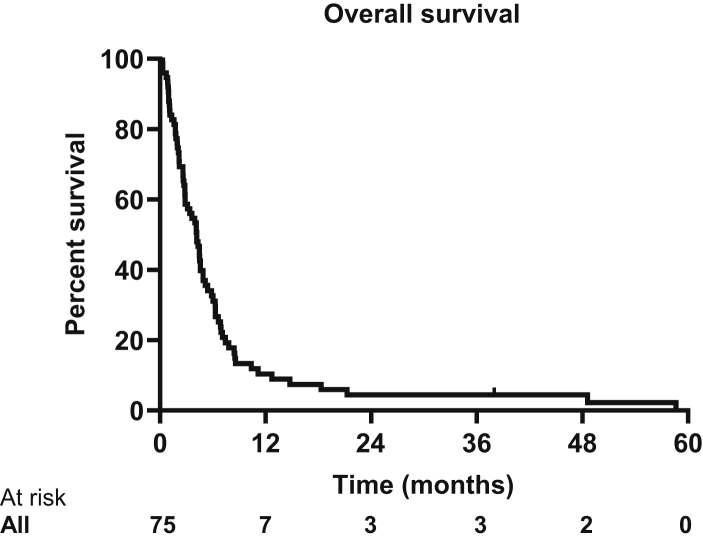
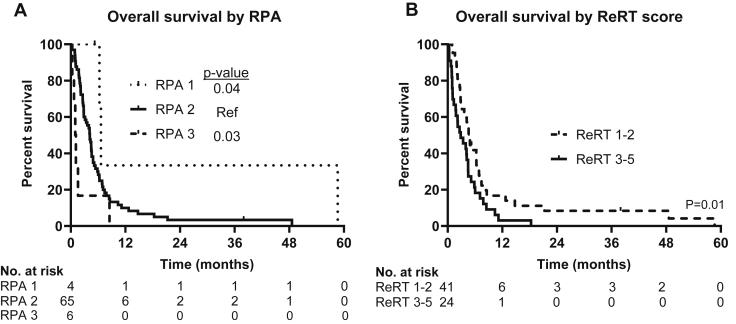
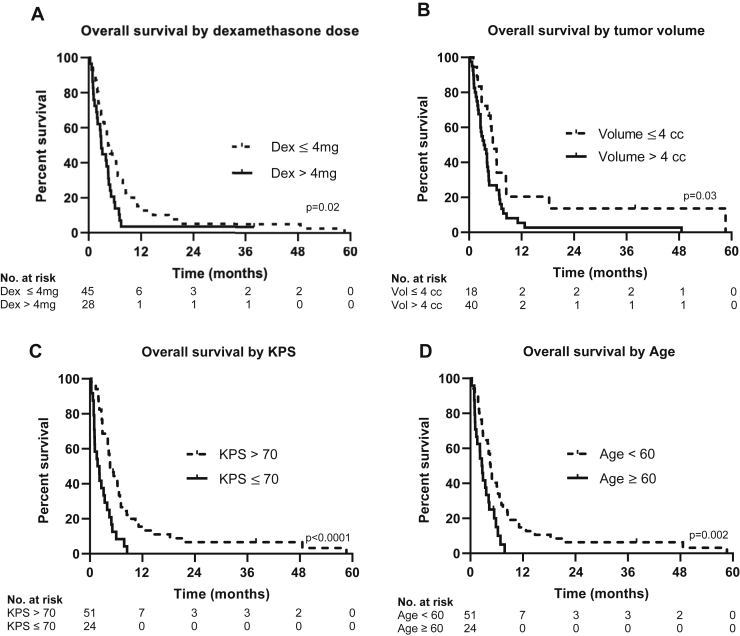
Seventy-five patients were treated with whole-brain PRDR radiation therapy. The median age was 54 (range, 26-72), the median Karnofsky performance status (KPS) was 80, and 86.7% had recursive partitioning analysis scores of 2. Thirty-two patients had over 10 metastases and 11 had leptomeningeal disease. The median overall survival was 4.1 months (range, 0.29-59.5 months) with a 1 year overall survival of 10.4%. Age, KPS, dexamethasone usage, and intracranial disease volume were significantly correlated with overall survival on multivariate analysis. A KPS ≤70 was associated with rapid death after radiation. The prognostic value of the ReRT score was validated. The most common acute toxicities were fatigue (23.1%) and headache (16.9%).
In this large cohort of patients with advanced intracranial metastases, PRDR achieves acceptable survival and may decrease toxicity associated with ReRT. PRDR is an easily implemented technique and is a viable treatment option for ReRT of brain metastases.
全脑放疗后复发性颅内转移瘤因其治疗相关的发病率不断上升而构成临床挑战。尽管立体定向放射外科的应用越来越广泛,但在某些情况下,全脑再程放疗(ReRT)仍然是合适的。在此,我们报告我们使用全脑脉冲低剂量率放射治疗(PRDR)的经验,该方法以0.067 Gy/分钟的较慢速率给予放射治疗,以潜在地增加亚致死性损伤修复并降低毒性。
分析了2001年1月1日至2019年3月接受全脑PRDR再程放疗的患者。PRDR再程放疗的中位剂量为26 Gy,分2 Gy分次给予,全脑总中位剂量为59.5 Gy。采用Cox回归分析进行多因素分析。采用Kaplan-Meier方法计算总生存期、无进展生存期,并评估再程放疗评分。采用二元逻辑回归评估与快速死亡相关的变量。
75例患者接受了全脑PRDR放射治疗。中位年龄为54岁(范围26 - 72岁),中位卡氏功能状态评分(KPS)为80分,86.7%的患者递归分区分析评分为2分。32例患者有超过10个转移灶,11例患者有软脑膜疾病。中位总生存期为4.1个月(范围0.29 - 59.5个月),1年总生存率为10.4%。多因素分析显示,年龄、KPS、地塞米松使用情况和颅内疾病体积与总生存期显著相关。KPS≤70与放疗后快速死亡相关。再程放疗评分的预后价值得到验证。最常见的急性毒性反应为疲劳(23.1%)和头痛(16.9%)。
在这一大型晚期颅内转移瘤患者队列中,PRDR取得了可接受的生存期,并可能降低与再程放疗相关的毒性。PRDR是一种易于实施的技术,是脑转移瘤再程放疗的可行治疗选择。