Wang Laureen Yi-Ting, Ng Gavin Yeow Ping
National University Heart Centre, National University Hospital Singapore, 5 Lower Kent Ridge Rd, Singapore 119074.
Eur Heart J Case Rep. 2020 Jun 30;4(FI1):1-6. doi: 10.1093/ehjcr/ytaa171. eCollection 2020 Oct.
COVID-19 infection is the most serious global public health crisis of the century. With no approved treatments against it, investigational treatments are being used despite limited safety data. Besides being at higher risk of complications of COVID-19 infection, patients with underlying cardiovascular disease are more likely to develop cardiac-related side effects of treatment. We present a case of sinus arrest with junctional escape related to lopinavir-ritonavir.
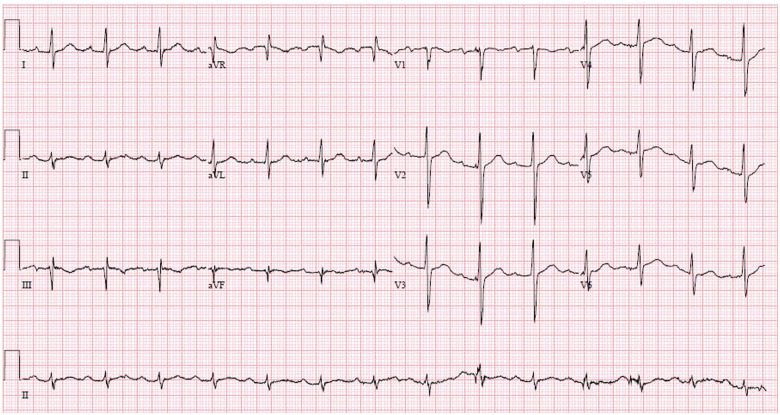
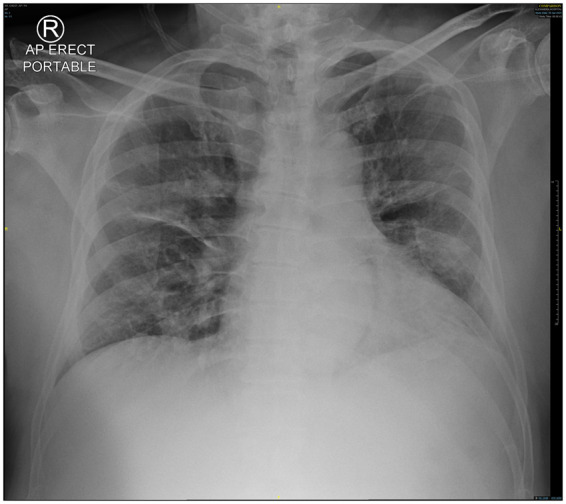
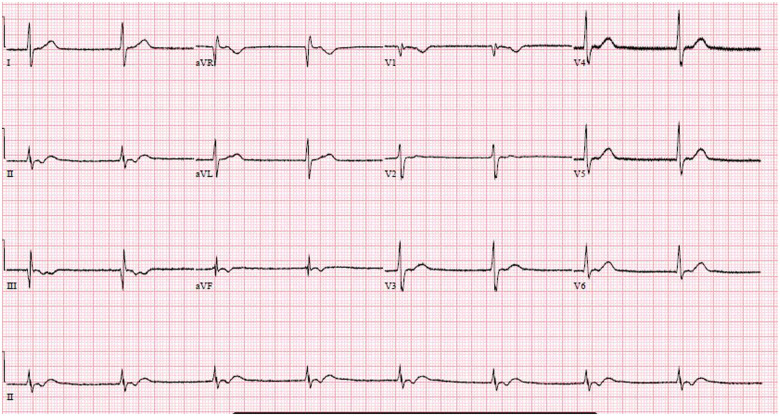
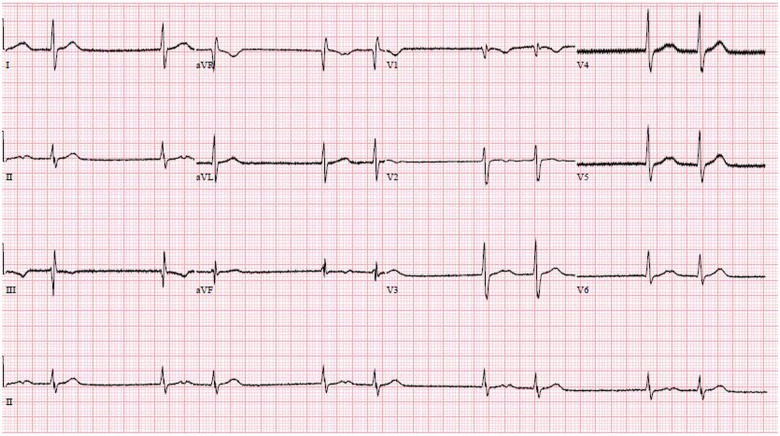
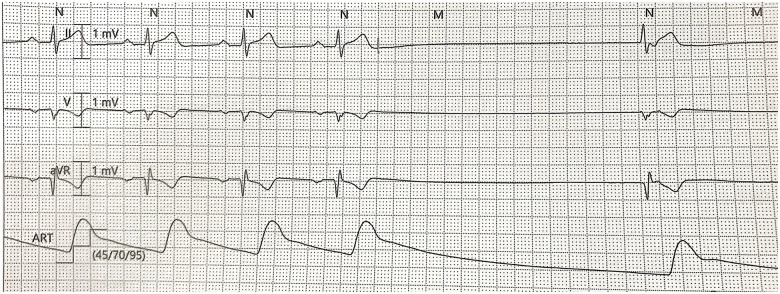
A 67-year-old man, with underlying stable ischaemic heart disease, acquired COVID-19 infection. He had a prolonged duration of fever and cough. He subsequently developed acute respiratory distress and required intensive care unit (ICU) care. Given his severe infection, he was started on lopinavir-ritonavir. Hydroxychloroquine was not used as he had a prolonged QTc interval. During observation in the ICU, the patient developed recurrent episodes of sinus arrest with junctional escape. Initial concerns were of myocarditis, but he had no ST-segment changes on ECG, with mild elevations of highly sensitive troponin I and a normal transthoracic echocardiogram. A multidisciplinary team discussion involving the intensivist, infectious disease physicians, and cardiologist; the decision was made to stop treatment with lopinavir-ritonavir. Within 48 h, the bradyarrhythmia resolved. The patient did not require transvenous and permanent pacemaker insertion.
Current efficacy and safety evidence of lopinavir-ritonavir as a treatment in COVID-19 patients is limited. Although uncommonly reported, those with underlying cardiovascular disease are at increased risk of bradyarrhythmia-related adverse effects of lopinavir-ritonavir. When initiating investigational therapies, especially in patients with cardiovascular conditions, adequate counselling and close monitoring are required.
新型冠状病毒肺炎(COVID-19)感染是本世纪最严重的全球公共卫生危机。由于尚无获批的针对该疾病的治疗方法,尽管安全性数据有限,但仍在使用试验性治疗方法。除了发生COVID-19感染并发症的风险较高外,患有潜在心血管疾病的患者更有可能出现治疗相关的心脏副作用。我们报告一例与洛匹那韦-利托那韦相关的窦性停搏伴交界性逸搏病例。
一名67岁男性,患有稳定的缺血性心脏病,感染了COVID-19。他发热和咳嗽持续时间较长。随后他出现急性呼吸窘迫,需要重症监护病房(ICU)治疗。鉴于其严重感染,开始使用洛匹那韦-利托那韦治疗。由于他的QTc间期延长,未使用羟氯喹。在ICU观察期间,患者出现反复的窦性停搏伴交界性逸搏发作。最初怀疑是心肌炎,但他的心电图无ST段改变,高敏肌钙蛋白I轻度升高,经胸超声心动图正常。经过包括重症监护医生、传染病医生和心脏病专家在内的多学科团队讨论;决定停止使用洛匹那韦-利托那韦治疗。在48小时内,缓慢性心律失常得到缓解。患者无需进行经静脉和永久性起搏器植入。
洛匹那韦-利托那韦作为COVID-19患者治疗药物的当前疗效和安全性证据有限。尽管报道较少,但患有潜在心血管疾病的患者发生洛匹那韦-利托那韦相关缓慢性心律失常不良反应的风险增加。在开始试验性治疗时,尤其是对于患有心血管疾病的患者,需要进行充分的咨询和密切监测。