Cizman Borut, Smith Helen T, Camejo Rodrigo Refoios, Casillas Linda, Dhillon Harjeet, Mu Fan, Wu Eric, Xie Jipan, Zuckerman Peter, Coyne Daniel
GlaxoSmithKline, Collegeville, PA.
GlaxoSmithKline, London, UK.
Kidney Med. 2020 Aug 10;2(5):589-599.e1. doi: 10.1016/j.xkme.2020.06.008. eCollection 2020 Sep-Oct.
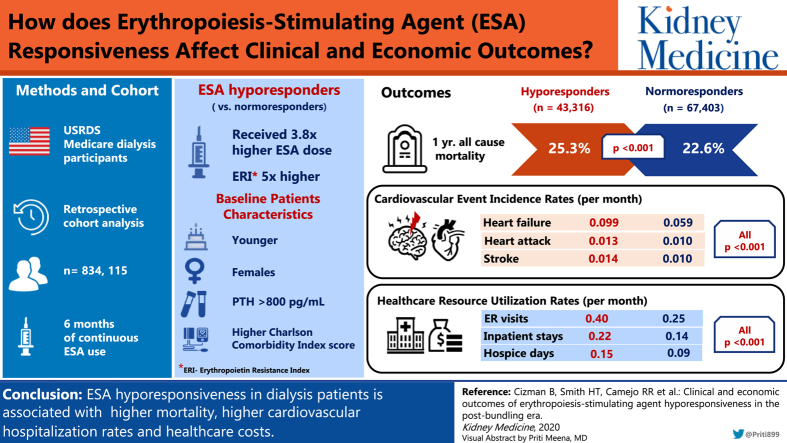
RATIONALE & OBJECTIVE: Since the change in erythropoiesis-stimulating agent (ESA) labeling and bundling of dialysis services in the United States, few studies have addressed the clinical importance of ESA hyporesponsiveness and none have considered health care resource use in this population. We aimed to further explore ESA hyporesponsiveness and its consequences.
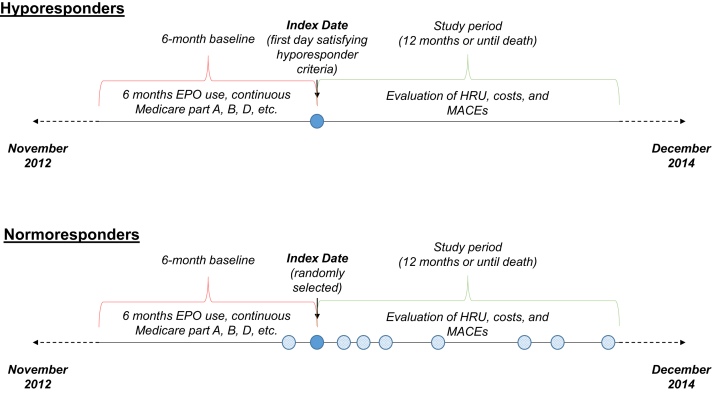
Retrospective observational cohort study.
SETTING & PARTICIPANTS: US Renal Data System Medicare participants receiving dialysis with a minimum 6 months of continuous ESA use from 2012 to 2014.
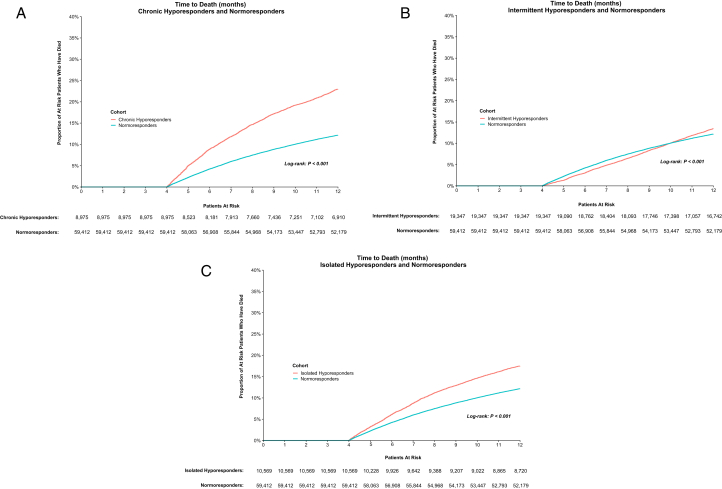
Erythropoietin resistance index (≥2.0 U/kg/wk/g/L) and ESA dose were used to identify ESA hyporesponders and hyporesponsive subgroups: isolated, intermittent, and chronic.
Associations between ESA responsiveness and mortality, cardiovascular hospitalization rates, and health care resource use were evaluated and compared across subgroups.
Baseline characteristics were compared using Wilcoxon rank sum tests for continuous variables and χ tests for categorical variables. Incidence rates of health care resource use were modeled using an unadjusted and adjusted generalized linear model.
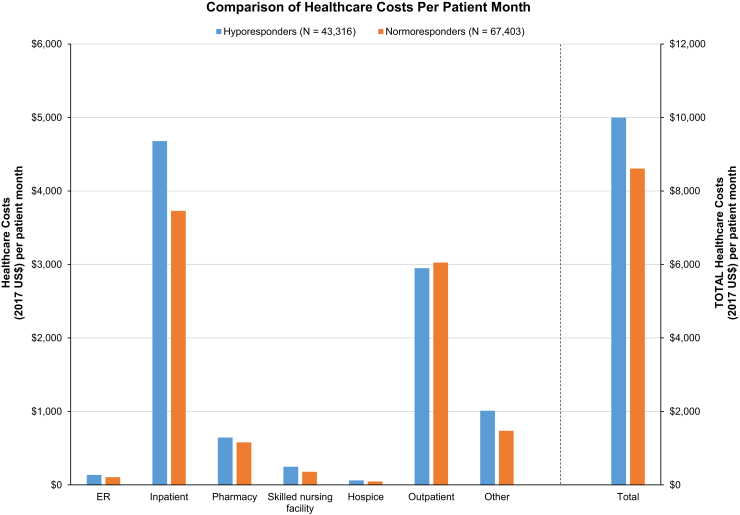
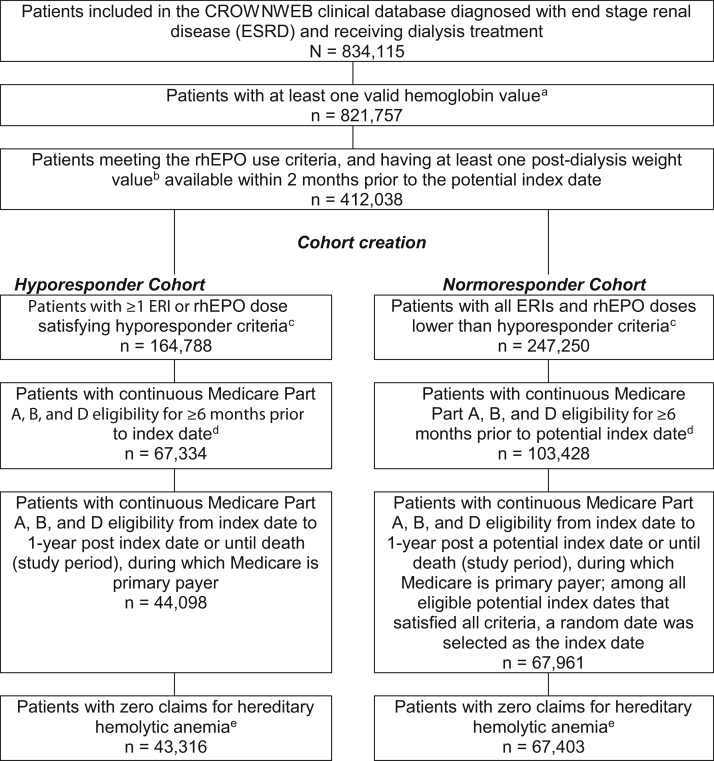
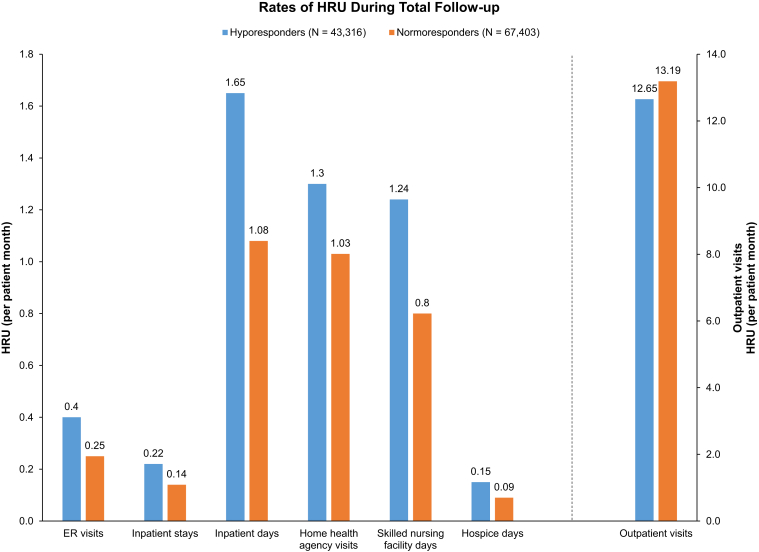
Of 834,115 dialysis patients in the CROWNWeb database, 38,891 ESA hyporesponders and 59,412 normoresponders met all inclusion criteria. Compared with normoresponders, hyporesponders were younger women, weighed less, and had longer durations of dialysis (all < 0.001). Hyporesponders received 3.8-fold higher ESA doses (mean, 94,831 U/mo) and erythropoietin resistance index was almost 5 times higher than in normoresponders. Hyporesponders had lower hemoglobin levels and parathyroid hormone levels > 800 pg/mL, and iron deficiency was present in 26.5% versus 10.9% in normoresponders. One-year mortality was higher among hypo- compared with normoresponders (25.3% vs 22.6%). Hyporesponders also had significantly higher rates of hospitalization for cardiovascular events, emergency department visits, inpatient stays, home health agency visits, skilled nursing facility, and hospice days.
Only US Medicare patients were included and different hyporesponder definitions may have influenced the results.
This study explored ESA hyporesponsiveness using new definitions and incorporated clinical and economic outcomes. It established that ESA-hyporesponsive dialysis patients had higher mortality, cardiovascular hospitalization rates, and health care costs as compared with ESA-normoresponsive patients.
自美国促红细胞生成素刺激剂(ESA)标签变更以及透析服务捆绑以来,很少有研究探讨ESA低反应性的临床重要性,且尚无研究考虑该人群的医疗资源使用情况。我们旨在进一步探究ESA低反应性及其后果。
回顾性观察队列研究。
美国肾脏数据系统医疗保险参与者,他们在2012年至2014年期间接受透析且至少连续使用ESA 6个月。
促红细胞生成素抵抗指数(≥2.0 U/kg/周/g/L)和ESA剂量用于识别ESA低反应者和低反应亚组:孤立性、间歇性和慢性。
评估并比较了ESA反应性与死亡率、心血管住院率以及医疗资源使用之间在各亚组中的关联。
使用Wilcoxon秩和检验比较连续变量的基线特征,使用χ检验比较分类变量的基线特征。使用未调整和调整后的广义线性模型对医疗资源使用的发生率进行建模。
在CROWNWeb数据库的834,115名透析患者中,38,891名ESA低反应者和59,412名正常反应者符合所有纳入标准。与正常反应者相比,低反应者为年轻女性,体重较轻,透析时间更长(均P < 0.001)。低反应者接受的ESA剂量高3.8倍(平均94,831 U/月),促红细胞生成素抵抗指数几乎是正常反应者的5倍。低反应者的血红蛋白水平较低,甲状旁腺激素水平> 800 pg/mL,且26.5%存在缺铁,而正常反应者为10.9%。低反应者的一年死亡率高于正常反应者(25.3%对22.6%)。低反应者的心血管事件住院率、急诊科就诊率、住院天数、家庭健康机构就诊率、熟练护理机构就诊率和临终关怀天数也显著更高。
仅纳入了美国医疗保险患者,不同的低反应者定义可能影响结果。
本研究使用新定义探究了ESA低反应性,并纳入了临床和经济结果。结果表明,与ESA正常反应的患者相比,ESA低反应的透析患者死亡率更高、心血管住院率更高且医疗成本更高。