Shindiapina Polina, Ahmed Elshafa H, Mozhenkova Anna, Abebe Tamrat, Baiocchi Robert A
Division of Hematology, Department of Internal Medicine, The Ohio State University, Columbus, OH, United States.
Comprehensive Cancer Center, The James Cancer Hospital and Solove Research Institute, The Ohio State University, Columbus, OH, United States.
Front Oncol. 2020 Sep 30;10:1723. doi: 10.3389/fonc.2020.01723. eCollection 2020.
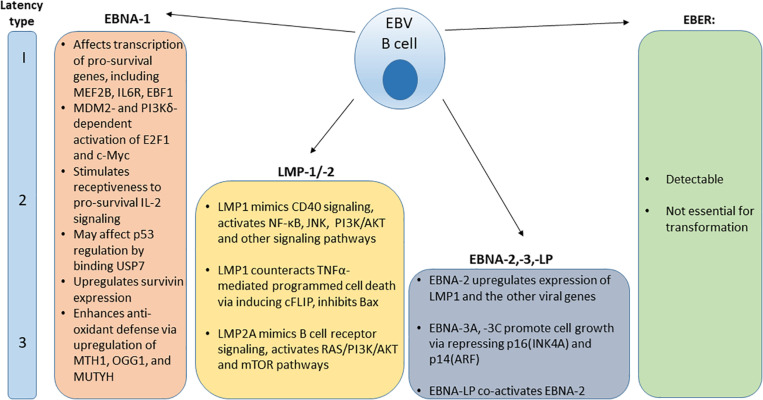
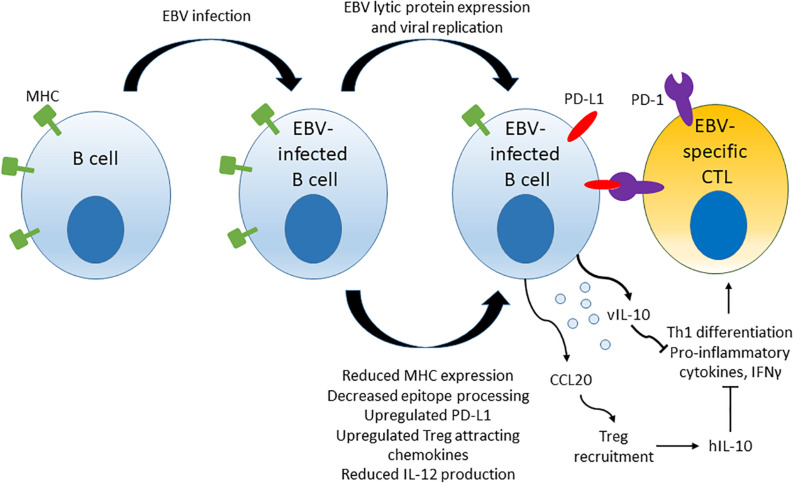
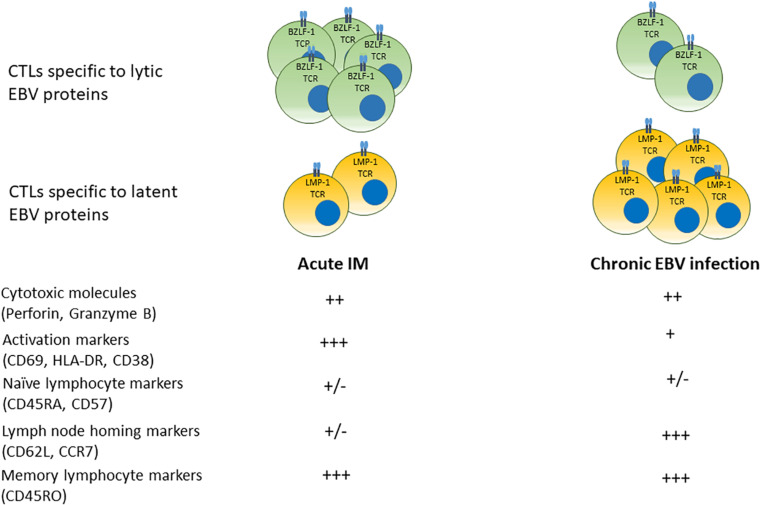
Epstein-Bar virus (EBV) can directly cause lymphoproliferative disease (LPD), including AIDS-defining lymphomas such as Burkitt's lymphoma and other non-Hodgkin lymphomas (NHL), as well as human immunodeficiency virus (HIV)-related Hodgkin lymphoma (HL). The prevalence of EBV in HL and NHL is elevated in HIV-positive individuals compared with the general population. Rates of incidence of AIDS-defining cancers have been declining in HIV-infected individuals since initiation of combination anti-retroviral therapy (cART) use in 1996. However, HIV-infected persons remain at an increased risk of cancers related to infections with oncogenic viruses. Proposed pathogenic mechanisms of HIV-related cancers include decreased immune surveillance, decreased ability to suppress infection-related oncogenic processes and a state of chronic inflammation marked by alteration of the cytokine profile and expanded numbers of cytotoxic T lymphocytes with down-regulated co-stimulatory molecules and increased expression of markers of senescence in the setting of treated HIV infection. Here we discuss the cooperation of EBV-infected B cell- and environment-associated factors that may contribute to EBV-related lymphomagenesis in HIV-infected individuals. Environment-derived lymphomagenic factors include impaired host adaptive and innate immune surveillance, cytokine dysregulation and a pro-inflammatory state observed in the setting of chronic, cART-treated HIV infection. B cell factors include distinctive EBV latency patterns and host protein expression in HIV-associated LPD, as well as B cell-stimulating factors derived from HIV infection. We review the future directions for expanding therapeutic approaches in targeting the viral and immune components of EBV LPD pathogenesis.
爱泼斯坦-巴尔病毒(EBV)可直接引发淋巴增殖性疾病(LPD),包括定义艾滋病的淋巴瘤,如伯基特淋巴瘤和其他非霍奇金淋巴瘤(NHL),以及与人类免疫缺陷病毒(HIV)相关的霍奇金淋巴瘤(HL)。与普通人群相比,HIV阳性个体中HL和NHL的EBV感染率有所升高。自1996年开始使用联合抗逆转录病毒疗法(cART)以来,HIV感染者中定义艾滋病的癌症发病率一直在下降。然而,HIV感染者患与致癌病毒感染相关癌症的风险仍然较高。HIV相关癌症的潜在致病机制包括免疫监视功能下降、抑制感染相关致癌过程的能力降低,以及在接受治疗的HIV感染情况下,以细胞因子谱改变、细胞毒性T淋巴细胞数量增加、共刺激分子下调和衰老标志物表达增加为特征的慢性炎症状态。在此,我们讨论EBV感染的B细胞与环境相关因素之间的协同作用,这些因素可能导致HIV感染者发生EBV相关淋巴瘤。环境来源的淋巴瘤发生因素包括宿主适应性和先天性免疫监视受损、细胞因子失调以及在慢性cART治疗的HIV感染情况下观察到的促炎状态。B细胞因素包括HIV相关LPD中独特的EBV潜伏模式和宿主蛋白表达,以及HIV感染衍生的B细胞刺激因素。我们回顾了在针对EBV LPD发病机制的病毒和免疫成分扩展治疗方法方面的未来方向。