Faculty of Biology, Medicine and Health, University of Manchester, Manchester, UK.
The Christie NHS Foundation Trust, Manchester, UK.
Obes Surg. 2021 Feb;31(2):554-563. doi: 10.1007/s11695-020-05052-8. Epub 2020 Oct 26.
There are limited data on the impact of bariatric surgery on microvascular complications of type 2 diabetes (T2D), particularly diabetic neuropathy. We assessed microvascular complications (especially neuropathy) in obese patients with T2D before and 12 months after bariatric surgery.
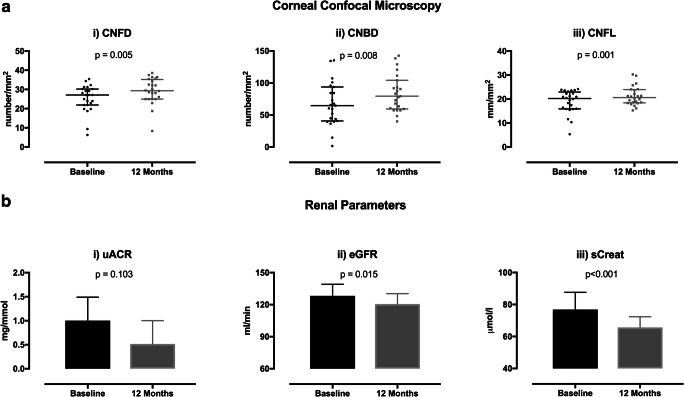
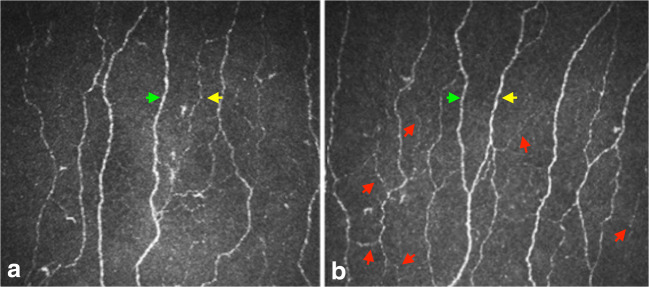
This was a prospective observational cohort study. Measurements of neuropathy symptom profile (NSP), neuropathy disability score (NDS), vibration (VPT), cold (CPT) and warm (WPT) perception thresholds, nerve conduction studies (NCS) and corneal confocal microscopy (CCM) to quantify corneal nerve fibre density (CNFD), branch density (CNBD) and fibre length (CNFL); urinary albumin/creatinine ratio (uACR), estimated glomerular filtration rate (eGFRcyst-creat) and retinal grading were taken.
Twenty-six (62% female; median age 52 years) obese patients with T2D were recruited. Body mass index (BMI) (47.2 to 34.5 kg/m; p < 0.001) decreased post-operatively. There were improvements in CNFD (27.1 to 29.2/mm; p = 0.005), CNBD (63.4 to 77.8/mm; p = 0.008), CNFL (20.0 to 20.2/mm; p = 0.001), NSP (3 to 0/38; p < 0.001) and eGFRcyst-creat (128 to 120 ml/min; p = 0.015) post-bariatric surgery. Changes in (Δ) triglycerides were independently associated with ΔCNFL (β = - 0.53; p = 0.024) and Δsystolic blood pressure (β = 0.62;p = 0.017), and %excess BMI loss (β = - 0.004; p = 0.018) were associated with ΔeGFRcyst-creat. There was no significant change in NDS, VPT, CPT, WPT, NCS, uACR or retinopathy status. Glomerular hyperfiltration resolved in 42% of the 12 patients with this condition pre-operatively.
Bariatric surgery results in improvements in small nerve fibres and glomerular hyperfiltration in obese people with T2D, which were associated with weight loss, triglycerides and systolic blood pressure, but with no change in retinopathy or uACR at 12 months.
关于减重手术对 2 型糖尿病(T2D)微血管并发症的影响,特别是糖尿病神经病变,目前数据有限。我们评估了肥胖 T2D 患者在减重手术前和手术后 12 个月的微血管并发症(尤其是神经病变)。
这是一项前瞻性观察队列研究。对神经病变症状谱(NSP)、神经病变残疾评分(NDS)、振动(VPT)、冷(CPT)和温(WPT)感觉阈值、神经传导研究(NCS)和角膜共聚焦显微镜(CCM)进行测量,以定量评估角膜神经纤维密度(CNFD)、分支密度(CNBD)和纤维长度(CNFL);测量尿白蛋白/肌酐比值(uACR)、估算肾小球滤过率(eGFRcyst-creat)和视网膜分级。
共招募了 26 名(62%为女性;中位年龄 52 岁)肥胖 T2D 患者。术后体重指数(BMI)(47.2 至 34.5kg/m2;p<0.001)下降。CNFD(27.1 至 29.2/mm;p=0.005)、CNBD(63.4 至 77.8/mm;p=0.008)、CNFL(20.0 至 20.2/mm;p=0.001)、NSP(3 至 0/38;p<0.001)和 eGFRcyst-creat(128 至 120ml/min;p=0.015)在减重手术后均有改善。(Δ)甘油三酯的变化与(Δ)CNFL(β=−0.53;p=0.024)和(Δ)收缩压(β=0.62;p=0.017)独立相关,而(%)超重体重减轻(β=−0.004;p=0.018)与(Δ)eGFRcyst-creat 相关。NDS、VPT、CPT、WPT、NCS、uACR 或视网膜病变状态无显著变化。术前肾小球高滤过的 12 名患者中有 42%在术后恢复正常。
减重手术可改善肥胖 T2D 患者的小神经纤维和肾小球高滤过,这与体重减轻、甘油三酯和收缩压有关,但在 12 个月时,视网膜病变或 uACR 没有变化。