University of Cambridge, Cambridge, UK.
Cambridge University Hospitals NHS Foundation Trust, Cambridge, UK.
Nat Microbiol. 2021 Jan;6(1):103-111. doi: 10.1038/s41564-020-00806-7. Epub 2020 Oct 26.
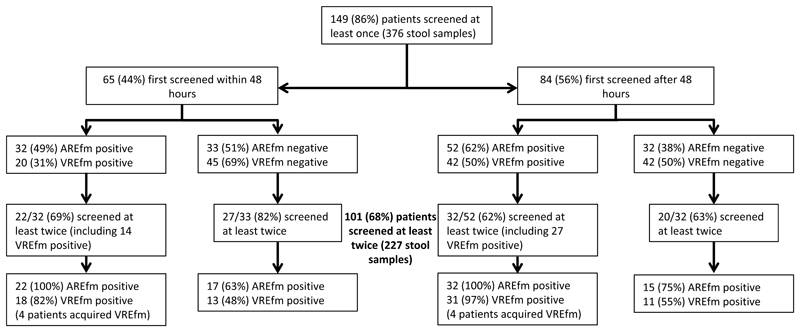
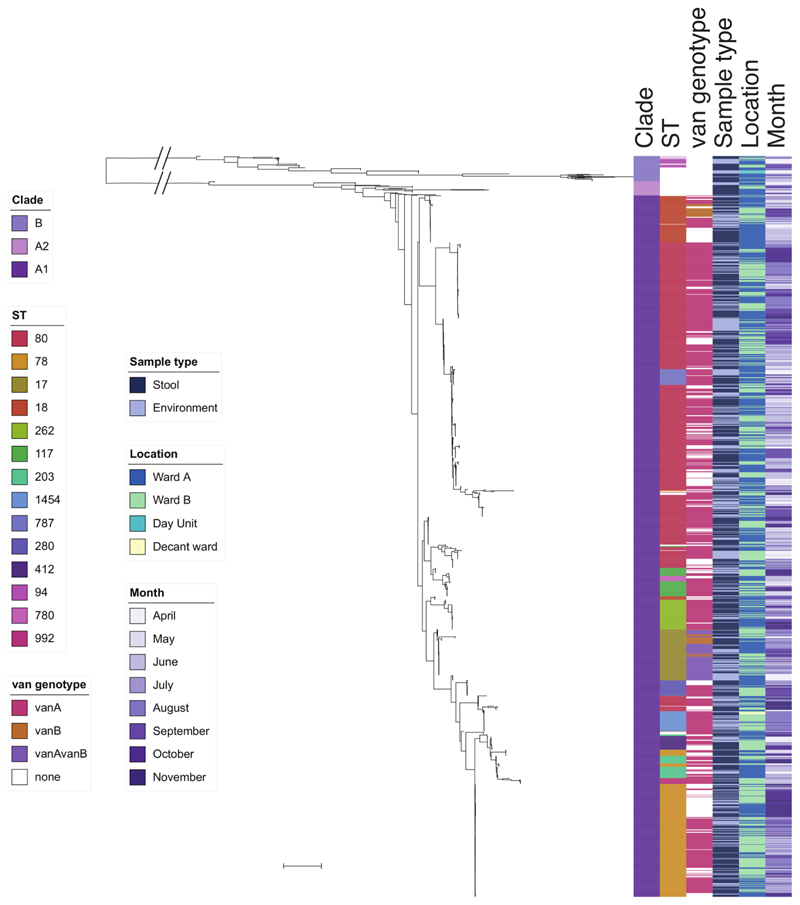
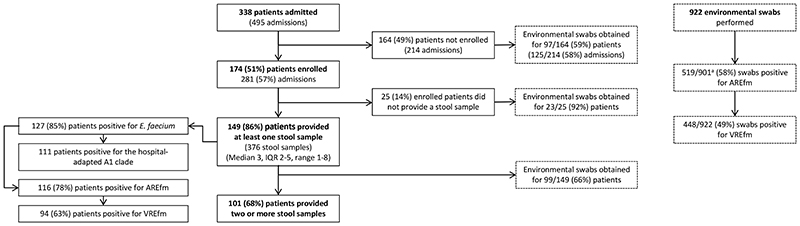
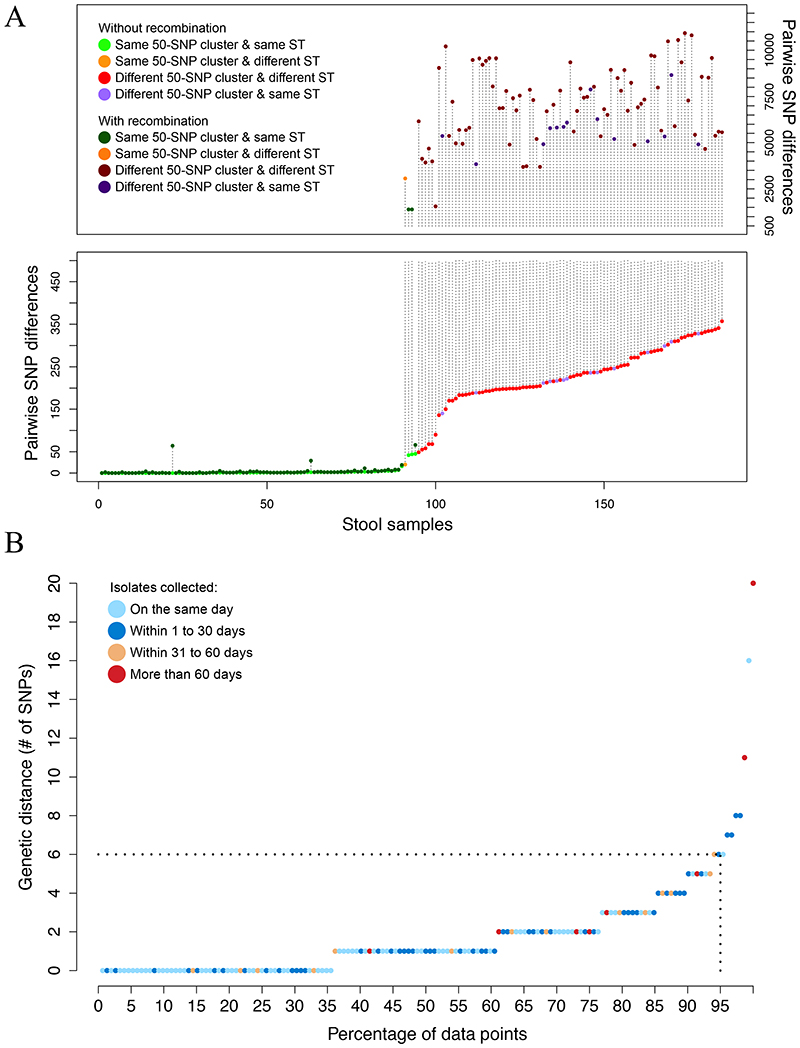
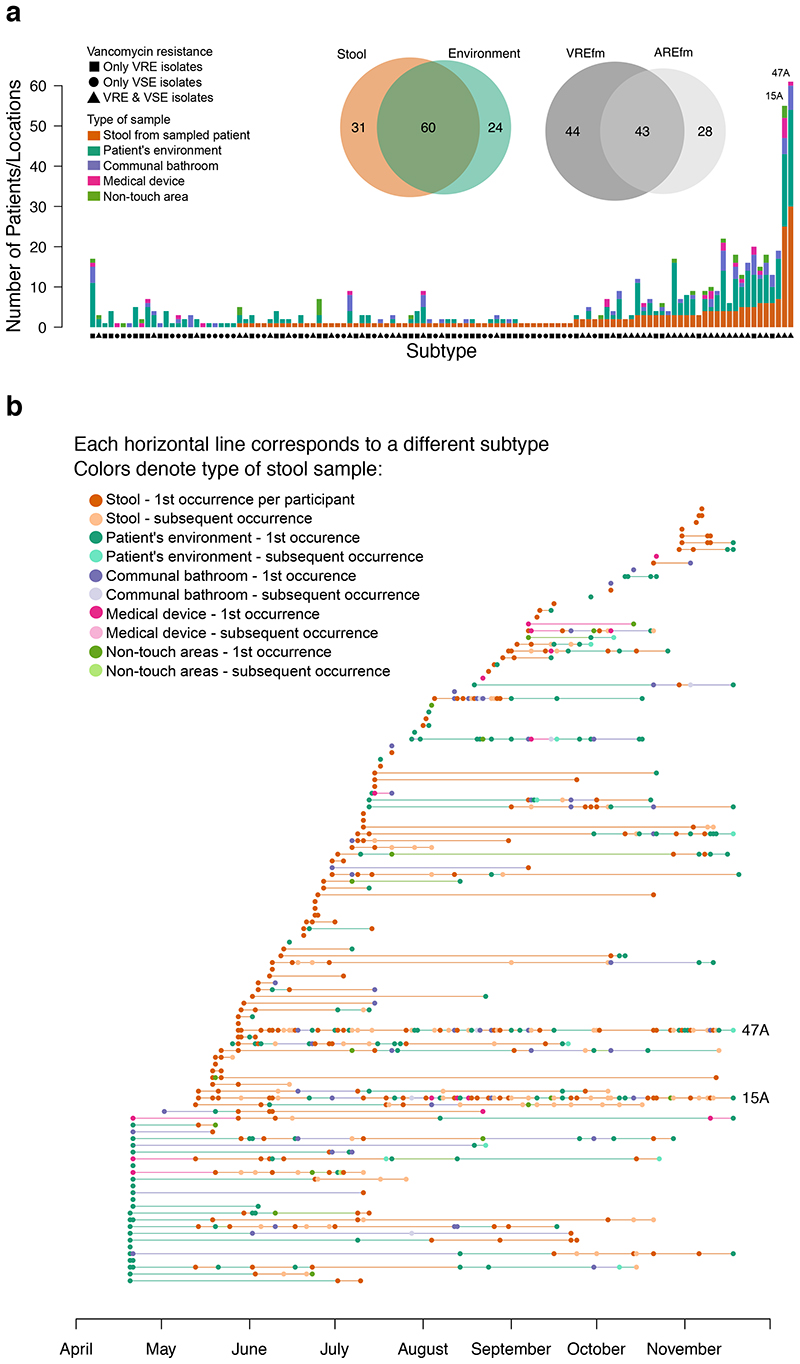
Nosocomial acquisition and transmission of vancomycin-resistant Enterococcus faecium (VREfm) is the driver for E. faecium carriage in hospitalized patients, which, in turn, is a risk factor for invasive infection in immunocompromised patients. In the present study, we provide a comprehensive picture of E. faecium transmission in an entire sampled patient population using a sequence-driven approach. We prospectively identified and followed 149 haematology patients admitted to a hospital in England for 6 months. Patient stools (n = 376) and environmental swabs (n = 922) were taken at intervals and cultured for E. faecium. We sequenced 1,560 isolates (1,001 stool, 559 environment) and focused our genomic analyses on 1,477 isolates (95%) in the hospital-adapted clade A1. Of 101 patients who provided two or more stool samples, 40 (40%) developed E. faecium carriage after admission based on culture, compared with 64 patients (63%) based on genomic analysis (73% VREfm). Half of 922 environmental swabs (447, 48%) were positive for VREfm. Network analysis showed that, of 111 patients positive for the A1 clade, 67 had strong epidemiological and genomic links with at least one other patient and/or their direct environment, supporting nosocomial transmission. Six patients (3.4%) developed an invasive E. faecium infection from their own gut-colonizing strain, which was preceded by nosocomial acquisition of the infecting isolate in half of these. Two informatics approaches (subtype categorization to define phylogenetic clusters and the development of an SNP cut-off for transmission) were central to our analyses, both of which will inform the future translation of E. faecium sequencing into routine outbreak detection and investigation. In conclusion, we showed that carriage and environmental contamination by the hospital-adapted E. faecium lineage were hyperendemic in our study population and that improved infection control measures will be needed to reduce hospital acquisition rates.
医院获得性传播的万古霉素耐药粪肠球菌(VREfm)是住院患者携带粪肠球菌的驱动因素,而粪肠球菌的携带则是免疫功能低下患者发生侵袭性感染的危险因素。在本研究中,我们采用序列驱动方法全面描绘了整个采样患者群体中粪肠球菌的传播情况。我们前瞻性地确定并随访了 149 名在英国一家医院住院 6 个月的血液科患者。每隔一段时间采集患者粪便(n=376)和环境拭子(n=922)进行粪肠球菌培养。我们共测序了 1560 株分离株(1001 株粪便,559 株环境),并将基因组分析重点放在医院适应的 A1 分支的 1477 株(95%)分离株上。在 101 名提供了两份或两份以上粪便样本的患者中,根据培养结果,有 40 名(40%)患者在入院后发生了粪肠球菌携带,而根据基因组分析结果(73%为 VREfm),则有 64 名(63%)患者发生了粪肠球菌携带。922 份环境拭子中有一半(447 份,48%)检测出 VREfm。网络分析显示,在 111 名 A1 分支阳性的患者中,有 67 名患者与至少一名其他患者及其直接环境具有强烈的流行病学和基因组联系,支持医院内传播。6 名(3.4%)患者从自身肠道定植菌株中发展为侵袭性粪肠球菌感染,其中一半患者在感染前先从医院获得了感染分离株。两种信息学方法(亚型分类以定义系统发育簇和开发用于传播的 SNP 截止值)是我们分析的核心,这两种方法都将有助于将粪肠球菌测序转化为常规暴发检测和调查。总之,我们发现,携带和环境污染的医院适应粪肠球菌谱系在我们的研究人群中高度流行,需要采取更好的感染控制措施来降低医院获得率。