Li Jian, Han Jing, Wang Yu, Mo Yunxian, Li Jibin, Xiang Jin, Li Zhiming, Zhou Jianhua, Wang Siyu
Department of Diagnostic & Interventional Ultrasound, Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangzhou, China.
Department of Medical Oncology, Sun Yat-sen University Cancer Center, State Key Laboratory of Oncology in South China, Collaborative Innovation Center for Cancer Medicine, Guangzhou, China.
Front Oncol. 2020 Oct 7;10:500153. doi: 10.3389/fonc.2020.500153. eCollection 2020.
Inadequate accuracy of ultrasound-guided core needle biopsy (US-CNB) urges further improvement for the diagnosis and management of lymphoma to meet with the practitioners' increased reliance on this mini-invasive approach.
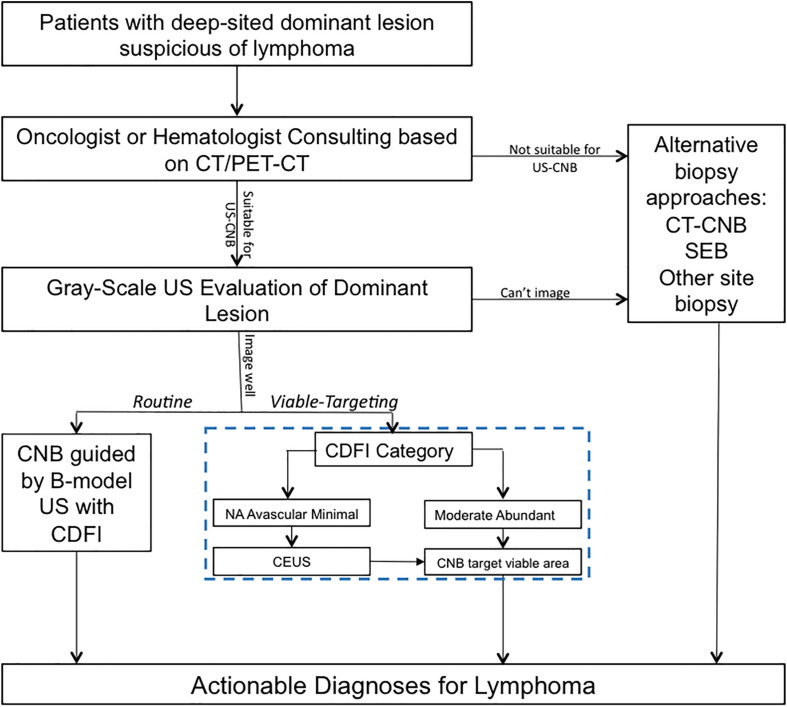
Data related to US-CNB of the deep-sited dominant lesions suspicious of lymphoma detected by computer tomography or positron-emission tomography/computer tomography for eligibility assessment of three prospective clinical trials were collected in advance. A retrospective analysis of the prospective data collection was performed, in which Viable-targeting US-CNB that Color Doppler flow imaging (CDFI) and/or contrast enhanced ultrasound (CEUS) were employed to select viable area for biopsy target compared with Routine US-CNB that routine procedure of evaluation and guidance using gray-scale ultrasound with CDFI in terms of the yield of clinically actionable diagnosis and safety, and determinants for the successful US-CNB that established an actionable diagnosis were explored. The establishment of final diagnosis was based on surgical pathology or medical response to therapy with follow-up at least 6 months.
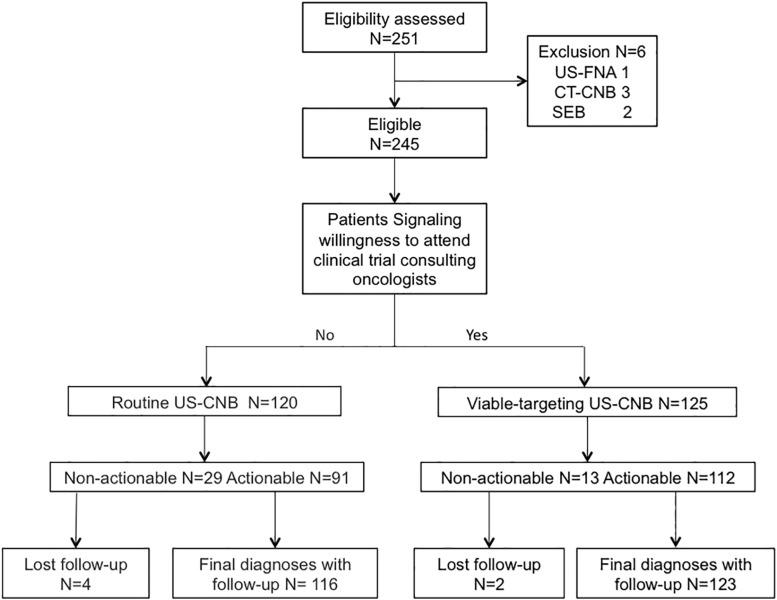
A total of 245 patients underwent Routine US-CNB ( = 120) or Viable-targeting US-CNB ( = 125), of which 91 (91/120, 75.8%) and 112 (112/125, 89.6%) were revealed with actionable diagnoses, respectively ( = 0.004, OR 0.846, 95% CI: 0.753-0.952). And 239 patients established final diagnoses. Diagnostic yields of actionable diagnosis according to the final diagnoses were 78.4% (91/116) and 91.1% (112/123) ( = 0.006, OR 0.554, 95% CI: 0.333-0.920), 82.6% (90/109) and 92.5% (111/120) for malignancy, 84.0% (84/100) and 91.8% (101/110) for lymphoma, 85.1% (80/94) and 92.3% (96/104) for Non-Hodgkin Lymphoma, 66.7% (4/6) and 83.3% (5/6) for Hodgkin Lymphoma in Routine and Viable-targeting CNB groups, respectively. No major complications were observed. Dominant lesions with actionable diagnosis in US-CNB were with higher FDG-avid Standardized Uptake Value. Binomial logistic regression revealed that actionable diagnosis of US-CNB was correlated with group and ancillary studies.
Viable-Targeting US-CNB was superior to routine US-CNB in term of the yield of actionable diagnosis for deep-sited dominant lesions suspicious of lymphoma, which demonstrated a potential to be the initial approach in this setting.
超声引导下粗针穿刺活检(US-CNB)的准确性不足,促使人们进一步改进淋巴瘤的诊断和管理方法,以满足从业者对这种微创方法日益增加的依赖。
预先收集了三项前瞻性临床试验中通过计算机断层扫描或正电子发射断层扫描/计算机断层扫描检测到的疑似淋巴瘤的深部主要病变的US-CNB相关数据,用于资格评估。对前瞻性数据收集进行回顾性分析,将采用彩色多普勒血流成像(CDFI)和/或超声造影(CEUS)选择活检目标的可行区域的靶向活组织超声引导下粗针穿刺活检(Viable-targeting US-CNB)与使用灰阶超声和CDFI进行评估和引导的常规程序的常规US-CNB在临床可行诊断的产量和安全性方面进行比较,并探索建立可行诊断的成功US-CNB的决定因素。最终诊断的建立基于手术病理或至少随访6个月的治疗医学反应。
共有245例患者接受了常规US-CNB(n = 120)或靶向活组织US-CNB(n = 125),其中分别有91例(91/120,75.8%)和112例(112/125,89.6%)获得了可行诊断(P = 0.004,OR 0.846,95% CI:0.753 - 0.952)。239例患者建立了最终诊断。根据最终诊断,可行诊断的诊断产量在常规和靶向活组织CNB组中分别为78.4%(91/116)和91.1%(112/123)(P = 0.006,OR 0.554,95% CI:0.333 - 0.920),恶性肿瘤为82.6%(90/109)和92.5%(111/120),淋巴瘤为84.0%(84/100)和91.8%(101/110),非霍奇金淋巴瘤为85.1%(80/94)和92.3%(96/104),霍奇金淋巴瘤为66.7%(4/6)和83.3%(5/6)。未观察到重大并发症。US-CNB中具有可行诊断的主要病变具有较高的FDG摄取标准化摄取值。二项逻辑回归显示,US-CNB的可行诊断与组和辅助研究相关。
在对疑似淋巴瘤的深部主要病变进行可行诊断的产量方面,靶向活组织US-CNB优于常规US-CNB,这表明它有可能成为这种情况下的初始方法。