OCHIN Inc, Portland, Oregon.
Department of Family Medicine, Oregon Health and Science University, Portland.
JAMA Netw Open. 2020 Oct 1;3(10):e2016852. doi: 10.1001/jamanetworkopen.2020.16852.
Responding to the substantial research on the relationship between social risk factors and health, enthusiasm has grown around social risk screening in health care settings, and numerous US health systems are experimenting with social risk screening initiatives. In the absence of standard social risk screening recommendations, some health systems are exploring using publicly available community-level data to identify patients who live in the most vulnerable communities as a way to characterize patient social and economic contexts, identify patients with potential social risks, and/or to target social risk screening efforts.
To explore the utility of community-level data for accurately identifying patients with social risks by comparing the social deprivation index score for the census tract where a patient lives with patient-level social risk screening data.
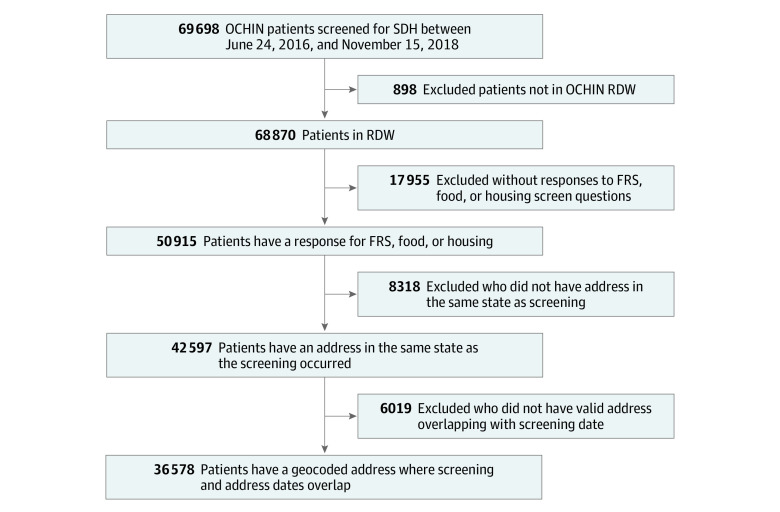
DESIGN, SETTING, AND PARTICIPANTS: Cross-sectional study using patient-level social risk screening data from the electronic health records of a national network of community health centers between June 24, 2016, and November 15, 2018, linked to geocoded community-level data from publicly available sources. Eligible patients were those with a recorded response to social risk screening questions about food, housing, and/or financial resource strain, and a valid address of sufficient quality for geocoding.
Social risk screening documented in the electronic health record.
Community-level social risk was assessed using census tract-level social deprivation index score stratified by quartile. Patient-level social risks were identified using food insecurity, housing insecurity, and financial resource strain screening responses.
The final study sample included 36 578 patients from 13 US states; 22 113 (60.5%) received public insurance, 21 181 (57.9%) were female, 17 578 (48.1%) were White, and 10 918 (29.8%) were Black. Although 6516 (60.0%) of those with at least 1 social risk factor were in the most deprived quartile of census tracts, patients with social risk factors lived in all census tracts. Overall, the accuracy of the community-level data for identifying patients with and without social risks was 48.0%.
Although there is overlap, patient-level and community-level approaches for assessing patient social risks are not equivalent. Using community-level data to guide patient-level activities may mean that some patients who could benefit from targeted interventions or care adjustments would not be identified.
随着对社会风险因素与健康之间关系的大量研究,人们对医疗保健环境中的社会风险筛查产生了浓厚的兴趣,许多美国医疗系统正在尝试社会风险筛查计划。由于缺乏标准的社会风险筛查建议,一些医疗系统正在探索使用公开的社区级数据来识别居住在最脆弱社区的患者,以此来描述患者的社会和经济背景,识别有潜在社会风险的患者,和/或确定社会风险筛查的重点。
通过将患者居住的普查区的社会剥夺指数评分与患者层面的社会风险筛查数据进行比较,探索使用社区级数据准确识别有社会风险的患者的效用。
设计、地点和参与者:这是一项使用全国社区卫生中心电子健康记录中的患者层面社会风险筛查数据进行的横断面研究,这些数据是在 2016 年 6 月 24 日至 2018 年 11 月 15 日之间收集的,并与公开来源的地理编码社区级数据相链接。合格患者是指那些记录了对食物、住房和/或经济资源紧张情况的社会风险筛查问题的回答,并且其地址质量足以进行地理编码。
记录在电子健康记录中的社会风险筛查。
通过按四分位数分层的普查区社会剥夺指数评分来评估社区层面的社会风险。通过食物无保障、住房无保障和经济资源紧张筛查反应来确定患者层面的社会风险。
最终的研究样本包括来自美国 13 个州的 36578 名患者;22113 名(60.5%)患者获得公共保险,21181 名(57.9%)为女性,17578 名(48.1%)为白人,10918 名(29.8%)为黑人。尽管有 6516 名(60.0%)至少有一种社会风险因素的患者处于普查区最贫困的四分位数,但有社会风险因素的患者居住在所有普查区。总体而言,社区级数据识别有和无社会风险患者的准确性为 48.0%。
尽管存在重叠,但患者层面和社区层面的评估患者社会风险的方法并不相同。使用社区级数据来指导患者层面的活动可能意味着,一些可能受益于针对性干预或护理调整的患者将无法被识别。