From the, Department of Emergency Medicine, Washington University in St. Louis School of Medicine, Emergency Care Research Core, St. Louis, MI, USA.
the, Department of Emergency Medicine, Icahn School of Medicine at Mount Sinai, New York, NY, USA.
Acad Emerg Med. 2021 Jan;28(1):19-35. doi: 10.1111/acem.14166. Epub 2020 Dec 12.
Older adult delirium is often unrecognized in the emergency department (ED), yet the most compelling research questions to overcome knowledge-to-practice deficits remain undefined. The Geriatric Emergency care Applied Research (GEAR) Network was organized to identify and prioritize delirium clinical questions.
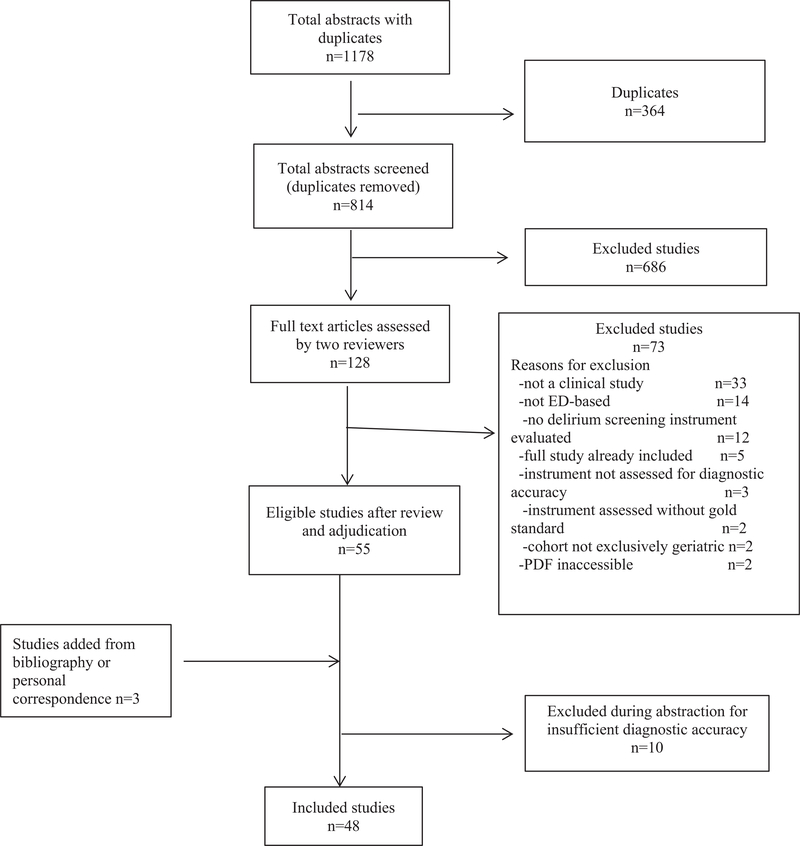
GEAR identified and engaged 49 transdisciplinary stakeholders including emergency physicians, geriatricians, nurses, social workers, pharmacists, and patient advocates. Adhering to Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Scoping Reviews, clinical questions were derived, medical librarian electronic searches were conducted, and applicable research evidence was synthesized for ED delirium detection, prevention, and management. The scoping review served as the foundation for a consensus conference to identify the highest priority research foci.
In the scoping review, 27 delirium detection "instruments" were described in 48 ED studies and used variable criterion standards with the result of delirium prevalence ranging from 6% to 38%. Clinician gestalt was the most common "instrument" evaluated with sensitivity ranging from 0% to 81% and specificity from 65% to 100%. For delirium management, 15 relevant studies were identified, including one randomized controlled trial. Some intervention studies targeted clinicians via education and others used clinical pathways. Three medications were evaluated to reduce or prevent ED delirium. No intervention consistently prevented or treated delirium. After reviewing the scoping review results, the GEAR stakeholders identified ED delirium prevention interventions not reliant on additional nurse or physician effort as the highest priority research.
Transdisciplinary stakeholders prioritize ED delirium prevention studies that are not reliant on health care worker tasks instead of alternative research directions such as defining etiologic delirium phenotypes to target prevention or intervention strategies.
老年人谵妄在急诊科(ED)常常未被识别,但克服知识-实践差距最引人关注的研究问题仍未确定。老年急诊应用研究(GEAR)网络的成立是为了确定和优先考虑谵妄临床问题。
GEAR 确定并邀请了 49 名跨学科利益相关者,包括急诊医师、老年科医生、护士、社会工作者、药剂师和患者权益维护者。根据系统评价和荟萃分析的首选报告项目进行了范围审查,从 ED 谵妄检测、预防和管理中提取了临床问题,进行了医学图书馆电子检索,并综合了适用的研究证据。该范围审查为确定最高优先级研究重点的共识会议提供了基础。
在范围审查中,48 项 ED 研究中描述了 27 种谵妄检测“工具”,并使用了不同的标准,导致谵妄患病率从 6%到 38%不等。临床医生的总体印象是最常用的“工具”,其敏感性从 0%到 81%不等,特异性从 65%到 100%不等。对于谵妄管理,确定了 15 项相关研究,包括一项随机对照试验。一些干预研究针对的是教育临床医生,而另一些则使用了临床路径。三种药物被评估用于减少或预防 ED 谵妄。没有干预措施能持续预防或治疗谵妄。在审查范围审查结果后,GEAR 利益相关者确定了不依赖于额外护士或医生工作量的 ED 谵妄预防干预措施作为最高优先级的研究。
跨学科利益相关者优先考虑不依赖于医护人员任务的 ED 谵妄预防研究,而不是其他研究方向,如定义谵妄表型以确定预防或干预策略。