Wang Lei, Tkhilaishvili Tamta, Trampuz Andrej
Center for Musculoskeletal Surgery, Charité-Universitätsmedizin Berlin, Corporate Member of Freie Universität Berlin, Humboldt-Universität zu Berlin and Berlin Institute of Health, 13353 Berlin, Germany.
Berlin-Brandenburg Center for Regenerative Therapies, Charité-Universitätsmedizin Berlin, 13353 Berlin, Germany.
Antibiotics (Basel). 2020 Oct 29;9(11):749. doi: 10.3390/antibiotics9110749.
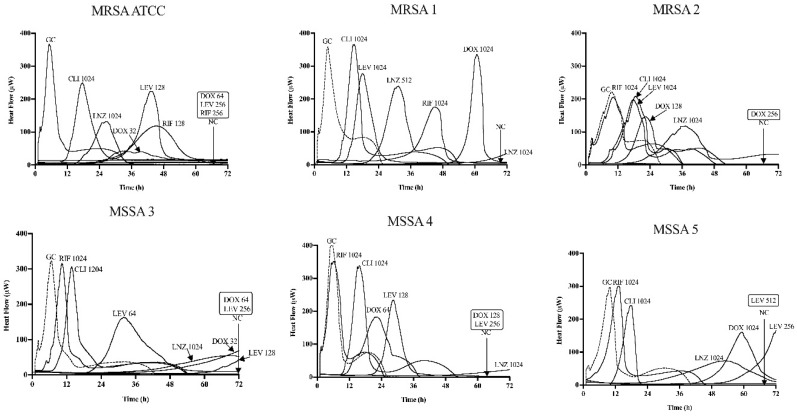
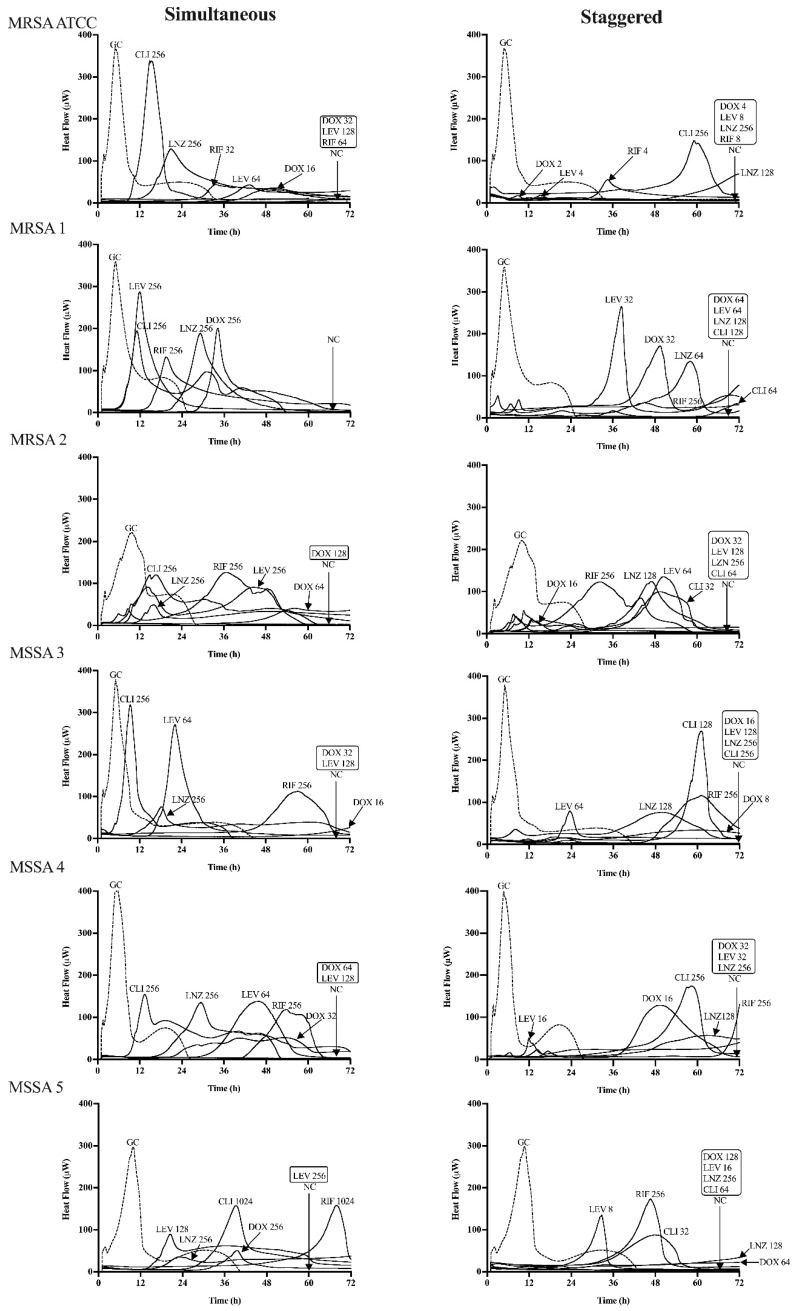
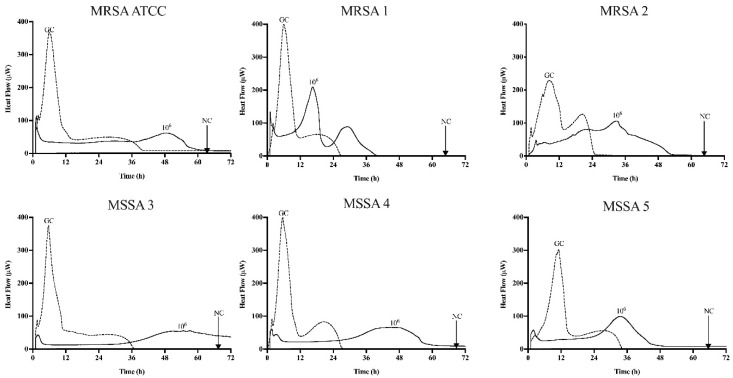
Effective antimicrobials are crucial for managing implant-associated bone infections (IABIs), particularly for infections due to rifampin-resistant (RRSA). Failure to remove the implant results in persistent infection; thus, prolonged suppressive antibiotic therapy may be a reasonable alternative. However, a high incidence of adverse events can necessitate the discontinuation of therapy. In this scenario, commercial bacteriophage Sb-1 combined with antibiotics is an option, showing a promising synergistic activity to facilitate the treatment of biofilm infections. Therefore, we evaluated the efficacy of the inhibitory activity of five antibiotics (doxycycline, levofloxacin, clindamycin, linezolid, and rifampin) alone or combined with phage Sb-1 (10 PFU/mL) in a simultaneous and staggered manner, to combat five clinical RRSA strains and the laboratory strain MRSA ATCC 43300 in 72 h by isothermal microcalorimetry. The synergistic effects were observed when phage Sb-1 (10 PFU/mL) combined with antibiotics had at least 2 log-reduction lower concentrations, represented by a fractional biofilm inhibitory concentration (FBIC) of <0.25. Among the antibiotics that we tested, the synergistic effect of all six strains was achieved in phage/doxycycline and phage/linezolid combinations in a staggered manner, whereas a distinctly noticeable improvement in inhibitory activity was observed in the phage/doxycycline combination with a low concentration of doxycycline. Moreover, phage/levofloxacin and phage/clindamycin combinations also showed a synergistic inhibitory effect against five strains and four strains, respectively. Interestingly, the synergistic inhibitory activity was also observed in the doxycycline-resistant and levofloxacin-resistant profile strains. However, no inhibitory activity was observed for all of the combinations in a simultaneous manner, as well as for the phage/rifampin combination in a staggered manner. These results have implications for alternative, combined, and prolonged suppressive antimicrobial treatment approaches.
有效的抗菌药物对于治疗植入物相关骨感染(IABIs)至关重要,尤其是对于耐利福平(RRSA)引起的感染。未能取出植入物会导致感染持续存在;因此,延长抑制性抗生素治疗可能是一种合理的替代方法。然而,不良事件的高发生率可能需要停止治疗。在这种情况下,商业噬菌体Sb-1与抗生素联合使用是一种选择,显示出有前景的协同活性,有助于治疗生物膜感染。因此,我们通过等温微量热法评估了五种抗生素(强力霉素、左氧氟沙星、克林霉素、利奈唑胺和利福平)单独或与噬菌体Sb-1(10 PFU/mL)同时及交错联合使用对五种临床RRSA菌株和实验室菌株MRSA ATCC 43300在72小时内的抑制活性效果。当噬菌体Sb-1(10 PFU/mL)与抗生素联合使用时,若浓度至少降低2个对数,以生物膜抑制浓度分数(FBIC)<0.25表示,则观察到协同效应。在我们测试的抗生素中,噬菌体/强力霉素和噬菌体/利奈唑胺组合以交错方式对所有六种菌株均实现了协同效应,而在低浓度强力霉素的噬菌体/强力霉素组合中观察到抑制活性有明显显著的提高。此外,噬菌体/左氧氟沙星和噬菌体/克林霉素组合分别对五种菌株和四种菌株也显示出协同抑制作用。有趣的是,在耐强力霉素和耐左氧氟沙星的菌株中也观察到了协同抑制活性。然而,同时联合使用的所有组合以及交错联合使用的噬菌体/利福平组合均未观察到抑制活性。这些结果对替代、联合和延长抑制性抗菌治疗方法具有启示意义。