Department of Internal Medicine, Section of Geriatric Medicine, Amsterdam Public Health Research Institute, Amsterdam University Medical Center, University of Amsterdam, Amsterdam, North Holland, The Netherlands.
Department of Global Public Health and Primary Care, University of Bergen, Bergen, Norway.
PLoS One. 2020 Nov 4;15(11):e0241132. doi: 10.1371/journal.pone.0241132. eCollection 2020.
Norway instituted a Coordination Reform in 2012 aimed at maximizing time at home by providing in-home care through community services. Dying in a hospital can be highly stressful for patients and families. Persons with dementia are particularly vulnerable to negative outcomes in hospital. This study aims to describe changes in the proportion of older adults with and without dementia dying in nursing homes, home, hospital and other locations over an 11-year period covering the reform.
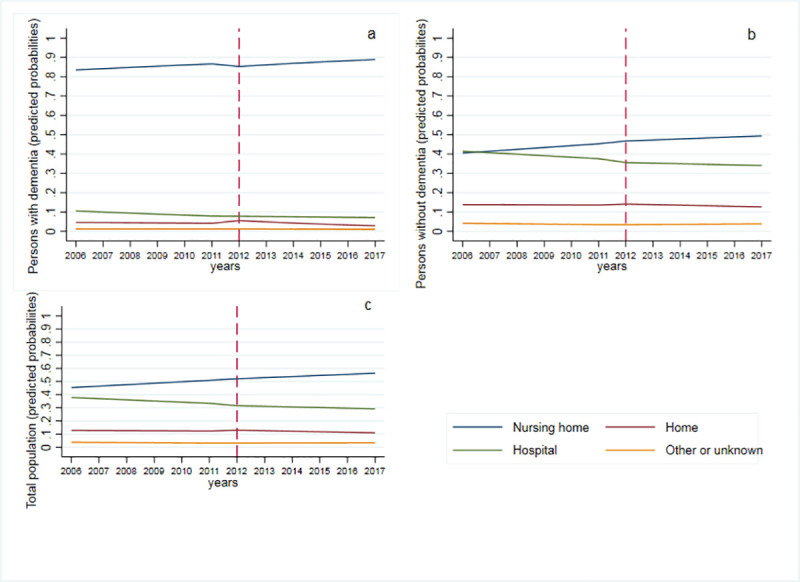
This is a repeated cross-sectional, population-level study using mortality data from the Norwegian Cause of Death Registry hosted by the Norwegian Institute of Public Health. Participants were Norwegian older adults 65 years or older with and without dementia who died from 2006 to 2017. The policy intervention was the 2012 Coordination Reform that increased care infrastructure into communities. The primary outcome was location of death listed as a nursing home, home, hospital or other location. The trend in the proportion of location of death, before and after the reform was estimated using an interrupted time-series analysis. All analyses were adjusted for sex and seasonality. Of the 417,862 older adult decedents, 61,940 (14.8%) had dementia identified on their death certificate. Nursing home deaths increased over time while hospital deaths decreased for the total population (adjusted Relative Risk Ratio (aRRR) 0.87, 95% CI 0.82-0.92) and persons with dementia (aRRR: 0.93, 95%CI 0.91-0.96) after reform implementation.
This study provides evidence that the 2012 Coordination Reform was associated with decreased older adults dying in hospital and increased nursing home death; however, the number of people dying at home did not change.
挪威于 2012 年实施了协调改革,旨在通过社区服务提供家庭护理,从而最大限度地延长在家时间。在医院去世会给患者和家属带来高度压力。痴呆症患者在医院尤其容易出现负面后果。本研究旨在描述在改革实施的 11 年期间,有无痴呆症的老年人在养老院、家中、医院和其他地点死亡的比例变化。
这是一项使用挪威公共卫生研究所主办的挪威死因登记处的死亡率数据进行的重复横断面、人群水平研究。参与者为 2006 年至 2017 年期间在挪威 65 岁及以上患有和不患有痴呆症的老年人。政策干预措施是 2012 年的协调改革,该改革增加了社区的护理基础设施。主要结局是列出养老院、家庭、医院或其他地点的死亡地点。使用中断时间序列分析估计改革前后死亡地点比例的趋势。所有分析均根据性别和季节性进行调整。在 417862 名老年死者中,有 61940 人(14.8%)在死亡证明上注明患有痴呆症。养老院死亡人数随着时间的推移而增加,而医院死亡人数则减少,总人群(调整后的相对风险比(aRRR)0.87,95%置信区间(CI)0.82-0.92)和患有痴呆症的人(aRRR:0.93,95%CI 0.91-0.96)在改革实施后。
本研究提供的证据表明,2012 年的协调改革与老年人在医院死亡人数减少和养老院死亡人数增加有关;然而,在家中死亡的人数并没有变化。