Medical Devices Unit, NHS Greater Glasgow and Clyde, Glasgow, UK.
Respiratory Medicine, Queen Elizabeth University Hospital, Glasgow, UK.
BMJ Open Respir Res. 2020 Nov;7(1). doi: 10.1136/bmjresp-2020-000710.
The COVID-19 pandemic has been characterised by significant in-hospital virus transmission and deaths among healthcare workers. Sources of in-hospital transmission are not fully understood, with special precautions currently reserved for procedures previously shown to generate aerosols (particles <5 μm). Pleural procedures are not currently considered AGPs (Aerosol Generating Procedures), reflecting a lack of data in this area.
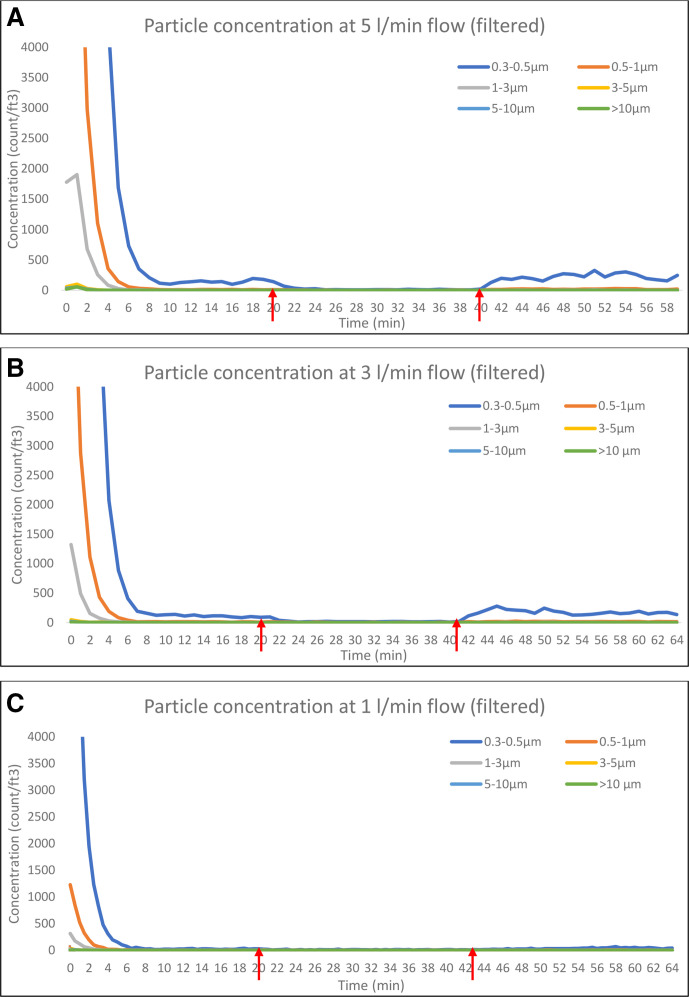
An underwater seal chest drain bottle (R54500, Rocket Medical UK) was set up inside a 60-litre plastic box and connected via an airtight conduit to a medical air supply. A multichannel particle counter (TSI Aerotrak 9310 Aerosol Monitor) was placed inside the box, allowing measurement of particle count/cubic foot (pc/ft) within six channel sizes: 0.3-0.5, 0.5-1, 1-3, 3-5, 5-10 and >10 μm. Stabilised particle counts at 1, 3 and 5 L/min were compared by Wilcoxon signed rank test; p values were Bonferroni-adjusted. Measurements were repeated with a simple anti-viral filter, designed using repurposed materials by the study team, attached to the drain bottle. The pressure within the bottle was measured to assess any effect of the filter on bottle function.
Aerosol emissions increased with increasing air flow, with the largest increase observed in smaller particles (0.3-3 μm). Concentration of the smallest particles (0.3-0.5 μm) increased from background levels by 700, 1400 and 2500 pc/ft at 1, 3 and 5 L/min, respectively. However, dispersion of particles of all sizes was effectively prevented by use of the viral filter at all flow rates. Use of the filter was associated with a maximum pressure rise of 0.3 cm HO after 24 hours of flow at 5 L/min, suggesting minimal impact on drain function.
A bubbling chest drain is a source of aerosolised particles, but emission can be prevented using a simple anti-viral filter. These data should be considered when designing measures to reduce in-hospital spread of SARS-CoV-2.
COVID-19 大流行的特点是医院内病毒传播和医护人员死亡显著。医院内传播的来源尚不完全清楚,目前特别注意先前显示会产生气溶胶(<5μm 的颗粒)的程序。胸膜程序目前不被认为是 AGPs(气溶胶生成程序),这反映了该领域缺乏数据。
将水下密封胸腔引流瓶(R54500,Rocket Medical UK)安装在一个 60 升的塑料盒内,并通过密封管道连接到医用空气供应。将多通道粒子计数器(TSI Aerotrak 9310 气溶胶监测器)放置在盒子内,允许在六个通道尺寸内测量粒子计数/立方英尺(pc/ft):0.3-0.5、0.5-1、1-3、3-5、5-10 和>10μm。通过 Wilcoxon 符号秩检验比较 1、3 和 5 L/min 时的稳定粒子计数;p 值采用 Bonferroni 校正。使用由研究小组重新利用材料设计的简单抗病毒过滤器重复测量。测量瓶内的压力以评估过滤器对瓶功能的任何影响。
气溶胶排放随空气流量增加而增加,最小颗粒(0.3-3μm)的增加最大。在 1、3 和 5 L/min 时,最小颗粒(0.3-0.5μm)的浓度分别从背景水平增加了 700、1400 和 2500 pc/ft。然而,在所有流速下使用病毒过滤器都有效地阻止了所有大小颗粒的分散。在 5 L/min 下 24 小时流量后,使用过滤器最大压力上升 0.3 cm HO,表明对引流功能的影响最小。
冒泡式胸腔引流是气溶胶化颗粒的来源,但使用简单的抗病毒过滤器可以防止排放。在设计减少 SARS-CoV-2 医院内传播的措施时应考虑这些数据。