Antoku Yoshibumi, Takemoto Masao, Suetsugu Fuminaga, Tsuchihashi Takuya
Cardiology, Cardiovascular Center, Steel Memorial Yawata Hospital, Kitakyushu, Japan.
Cardiology and Internal Medicine, Suetsugu Clinic, Kitakyushu, Japan.
JMA J. 2020 Jul 15;3(3):280-283. doi: 10.31662/jmaj.2020-0018. Epub 2020 Jun 19.
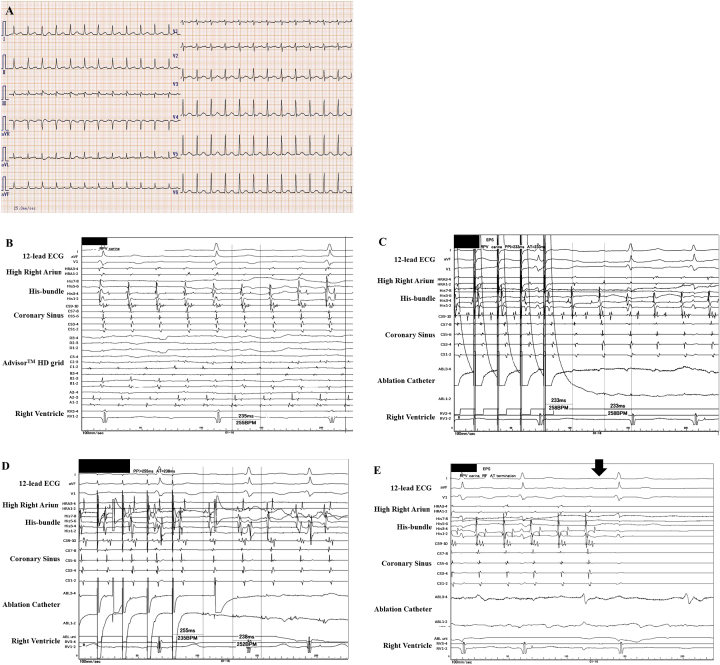
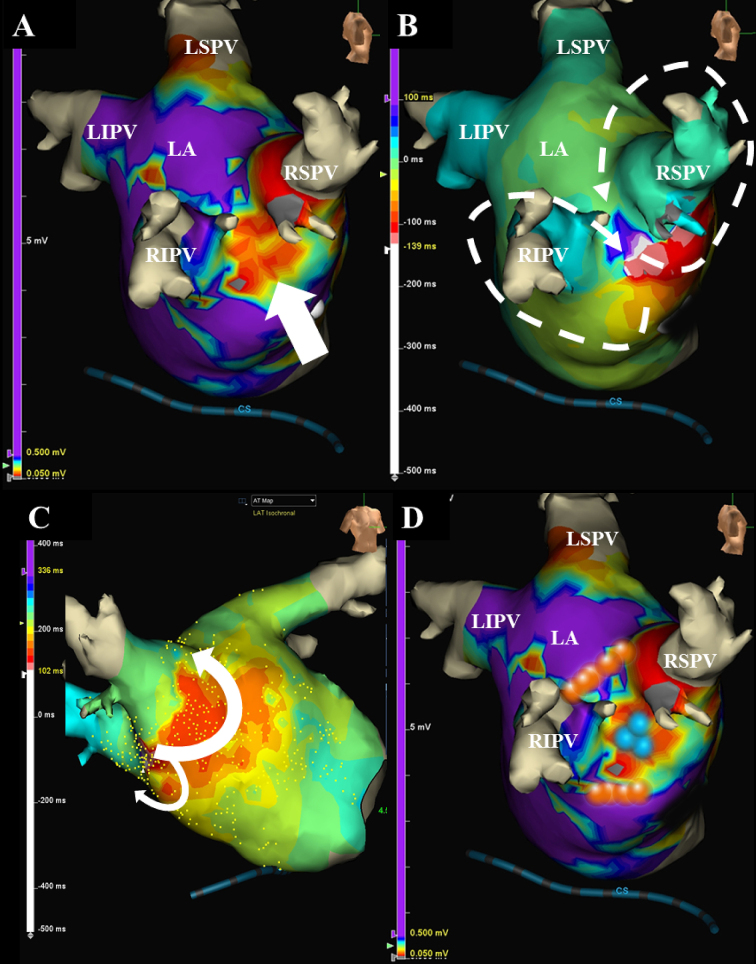
A 66-year-old female, whom received a pulmonary vein (PV) isolation (PVAI) with linear ablation of the carina lines between the superior and inferior PVs of both the right and left PVs for atrial fibrillation (AF), was admitted to receive a radiofrequency catheter ablation (RFCA) of symptomatic drug-refractory atrial tachycardia (AT). The EnSite analysis by the Advisor HD Grid catheter during the AT could easily detect that the carina between the right superior and inferior PVs exhibited a low voltage area (< 0.5 mV), in addition to the fact that the electrical activation turned around the right PVs in a figure 8, even though mapping was performed during AT. This AT was steadily terminated, after commencing the radiofrequency energy delivery to the carina of the right PVs.
一名66岁女性,因心房颤动(AF)接受了肺静脉(PV)隔离(PVAI)及左右肺静脉上下肺静脉之间隆突线的线性消融,现因症状性药物难治性房性心动过速(AT)入院接受射频导管消融(RFCA)。在AT发作期间,使用Advisor HD Grid导管进行的EnSite分析很容易检测到,即使在AT发作期间进行了标测,右肺静脉上下肺静脉之间的隆突仍显示出低电压区域(<0.5 mV),此外电活动在右肺静脉周围呈8字形折返。在开始对右肺静脉隆突进行射频能量输送后,该AT被稳定终止。