Department of Urology, The First Hospital of China Medical University, Shenyang 110001, Liaoning, China.
Department of Dermatology, The First Hospital of China Medical University, Shenyang 110001, Liaoning, China.
Aging (Albany NY). 2020 Nov 5;12(21):21854-21873. doi: 10.18632/aging.104001.
Papillary renal cell carcinoma (PRCC) accounts for 15% of all renal cell carcinomas. The molecular mechanisms of renal papillary cell carcinoma remain unclear, and treatments for advanced disease are limited.
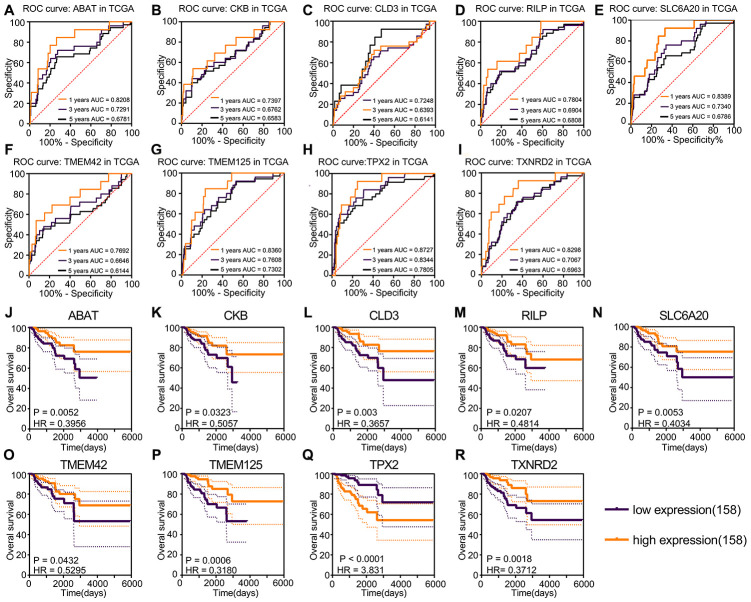
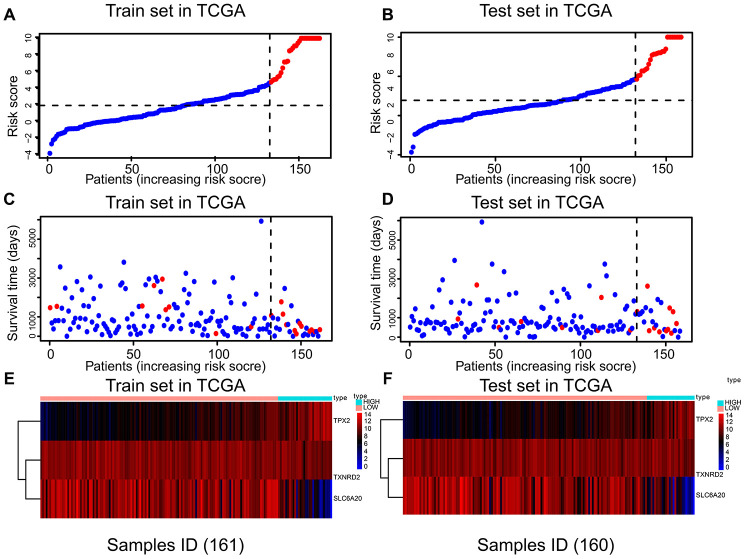
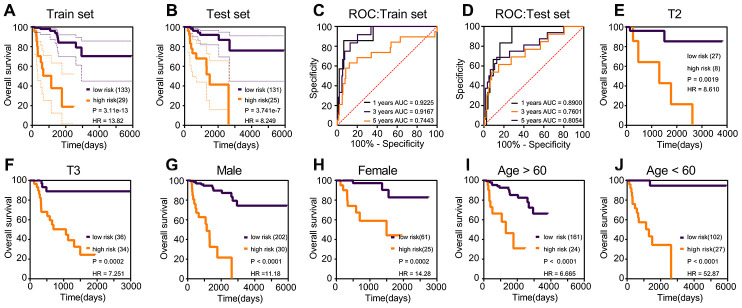
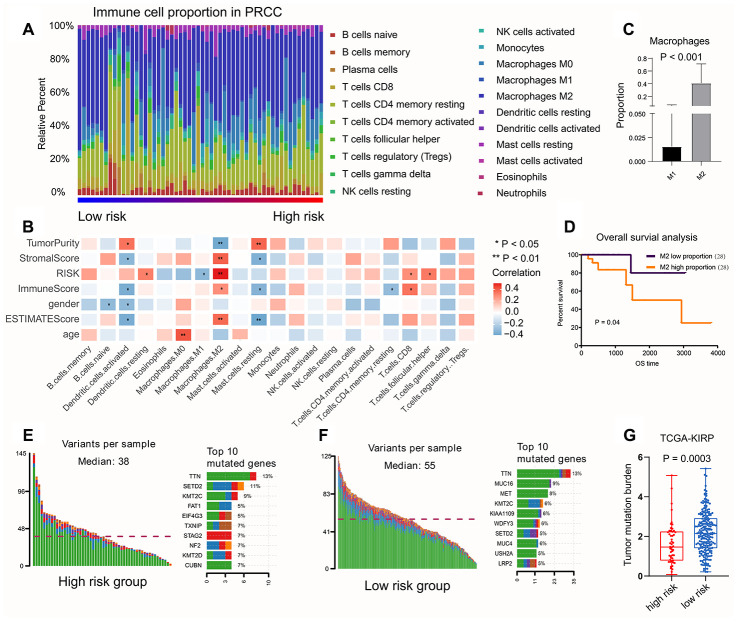
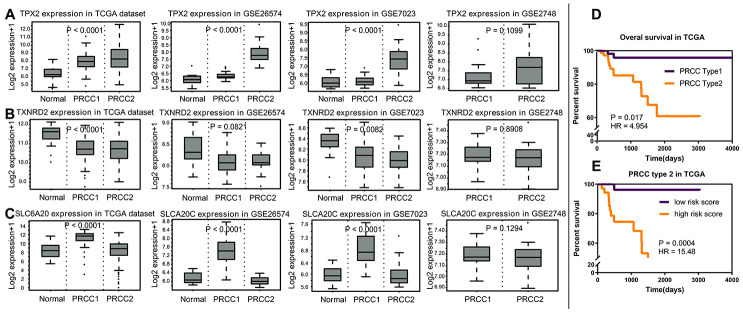
We built the computing model as follows: Risk score = 1.806 * - 0.355 * - 0.805 * . The 3-year AUC of overall survival was 0.917 in the training set (147 PRCC samples) and 0.760 in the test set (142 PRCC samples). Based on the robust model, M2 macrophages showed positive correlation with risk score, while M1 macrophages were the opposite. PRCC patients with low risk score showed higher tumor mutation burden. is a risk factor, and co-expression factors were enriched in cell proliferation and cancer-related pathways. Finally, the proliferation and invasion of PRCC cell line were decreased in the reduced group, and the differential expression was identified. is a potential risk biomarker which involved in cell proliferation in PRCC.
We conducted a study to develop a three gene model for predicting prognosis in patients with papillary renal cell carcinoma. Our findings may provide candidate biomarkers for prognosis that have important implications for understanding the therapeutic targets of papillary renal cell carcinoma.
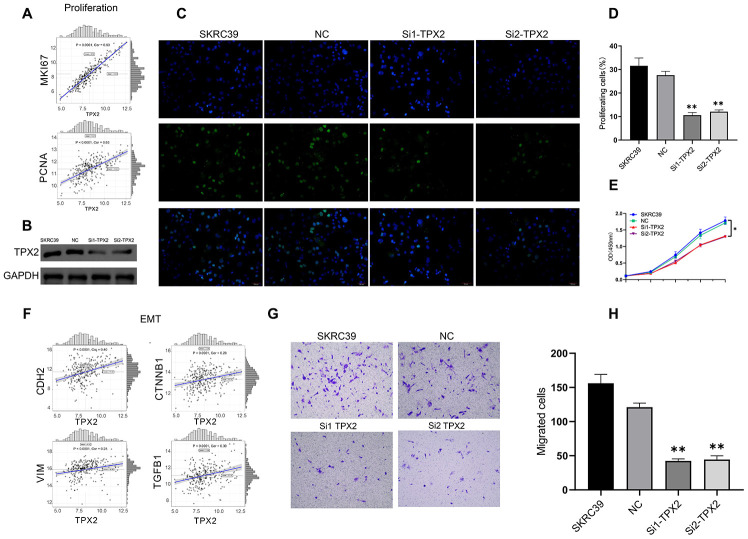
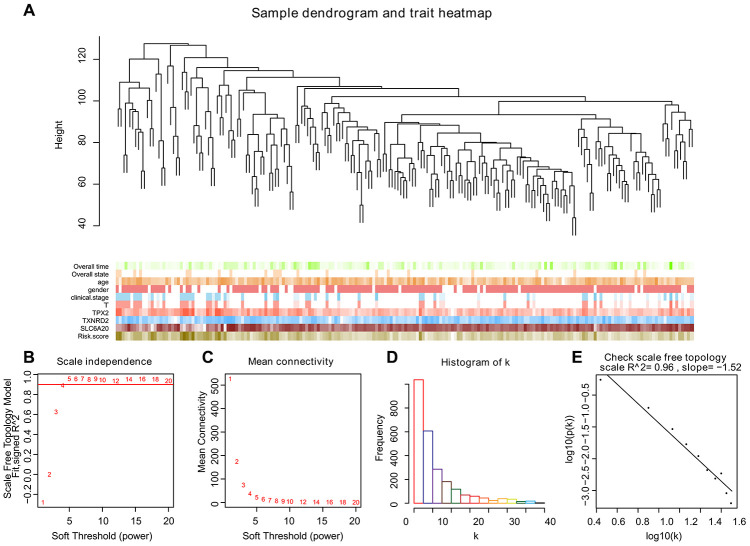
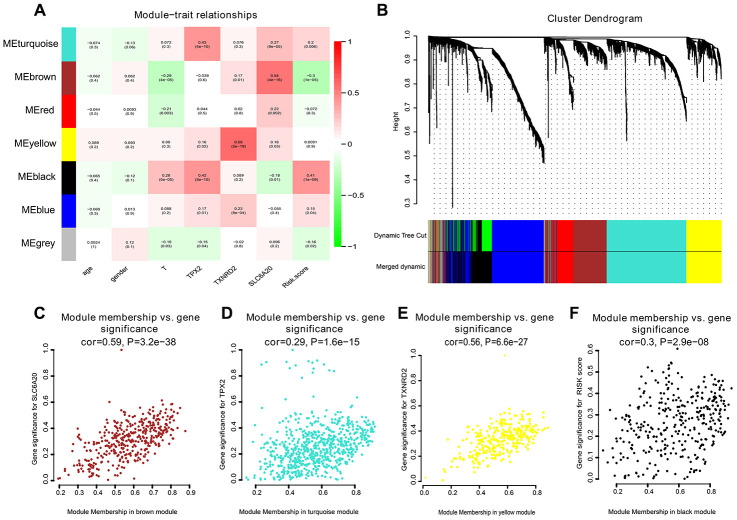
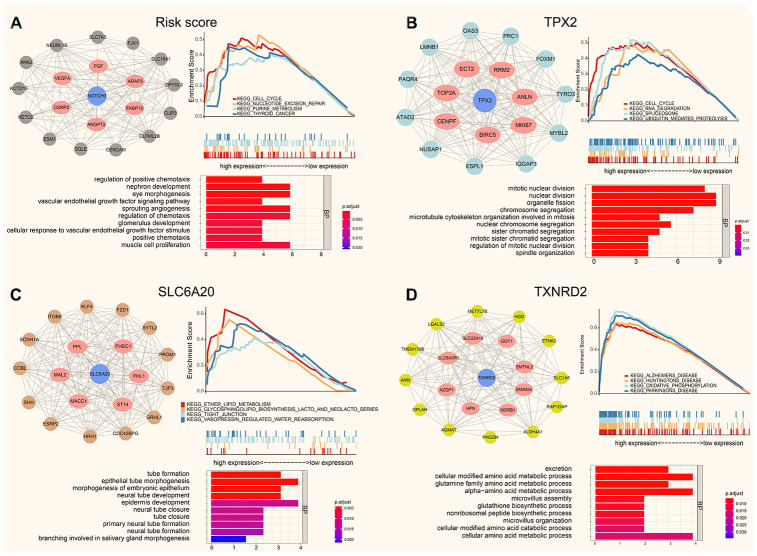
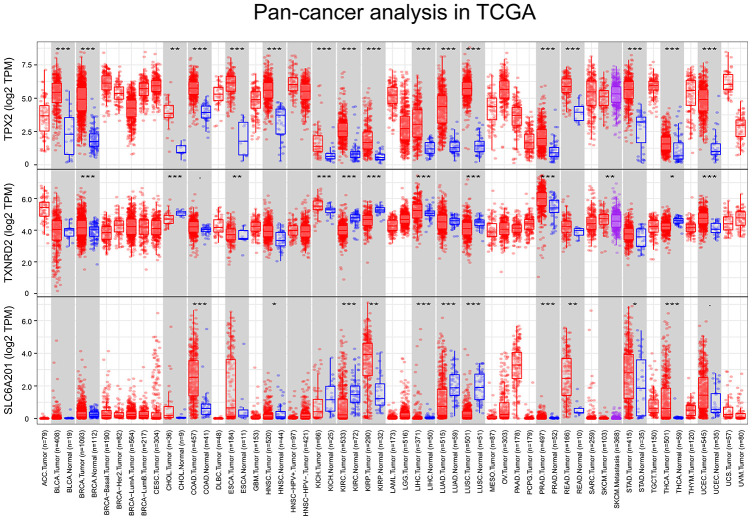
Gene expression matrix and clinical data were obtained from TCGA (The Cancer Genome Atlas), GSE26574, GSE2048, and GSE7023. Prognostic factors were identified using "survival" and "rbsurv" packages, and a risk score was constructed using Multivariate Cox regression analysis. The co-expression networks of the factors in model were constructed using the "WGCNA" package. The co-expression genes of factors were enriched and displayed the biological process. Based on this robust risk model, immune cells infiltration proportions and tumor mutation burdens were compared between risk groups. Subsequently, using the PRCC cell line, the role of TPX2 was determined by Cell proliferation assay, 5-Ethynyl-20-deoxyuridine assay and Transwell assay.
乳头状肾细胞癌(PRCC)占所有肾细胞癌的 15%。肾乳头状细胞癌的分子机制尚不清楚,晚期疾病的治疗方法有限。
我们构建了如下计算模型:风险评分=1.806×-0.355×-0.805×。在训练集(147 个 PRCC 样本)中,总生存的 3 年 AUC 为 0.917,在测试集(142 个 PRCC 样本)中为 0.760。基于稳健模型,M2 巨噬细胞与风险评分呈正相关,而 M1 巨噬细胞则相反。低风险评分的 PRCC 患者具有更高的肿瘤突变负担。是一个风险因素,共表达因子在细胞增殖和癌症相关途径中富集。最后,在 减少的组中,PRCC 细胞系的增殖和侵袭能力降低,并且鉴定出差异表达。是涉及 PRCC 细胞增殖的潜在风险生物标志物。
我们进行了一项研究,以开发一种用于预测乳头状肾细胞癌患者预后的三个基因模型。我们的研究结果可能为预后提供候选生物标志物,这对于理解乳头状肾细胞癌的治疗靶点具有重要意义。
从 TCGA(癌症基因组图谱)、GSE26574、GSE2048 和 GSE7023 中获取基因表达矩阵和临床数据。使用“survival”和“rbsurv”包识别预后因素,并使用多变量 Cox 回归分析构建风险评分。使用“WGCNA”包构建模型中因素的共表达网络。对模型中因素的共表达基因进行富集并显示生物过程。基于这一稳健的风险模型,比较风险组之间的免疫细胞浸润比例和肿瘤突变负担。随后,使用 PRCC 细胞系,通过细胞增殖测定、5-乙炔基-20-脱氧尿苷测定和 Transwell 测定确定 TPX2 的作用。