Alqalyoobi Shehabaldin, Fernández Pérez Evans R, Oldham Justin M
Division of Pulmonary, Critical Care and Sleep Medicine, Department of Medicine, East Carolina University-Brody School of Medicine, Greenville, North Carolina, USA.
Present address: Internal Medicine - Pulmonary, Critical Care, and Sleep Medicine, Brody School of Medicine, Mail Stop 628, 3E-149, Greenville, NC, 27834, USA.
BMC Pulm Med. 2020 Nov 7;20(1):289. doi: 10.1186/s12890-020-01328-y.
Idiopathic pulmonary fibrosis (IPF) is a devastating condition characterized by progressive lung function decline and early mortality. While early accurate diagnosis is essential for IPF treatment, data evaluating the impact of hospital academic status on IPF-related mortality remains limited. Here we examined in-hospital mortality trends for patients with IPF from 2013 to 2017. We hypothesized that in-hospital IPF mortality would be influenced by hospital academic setting.
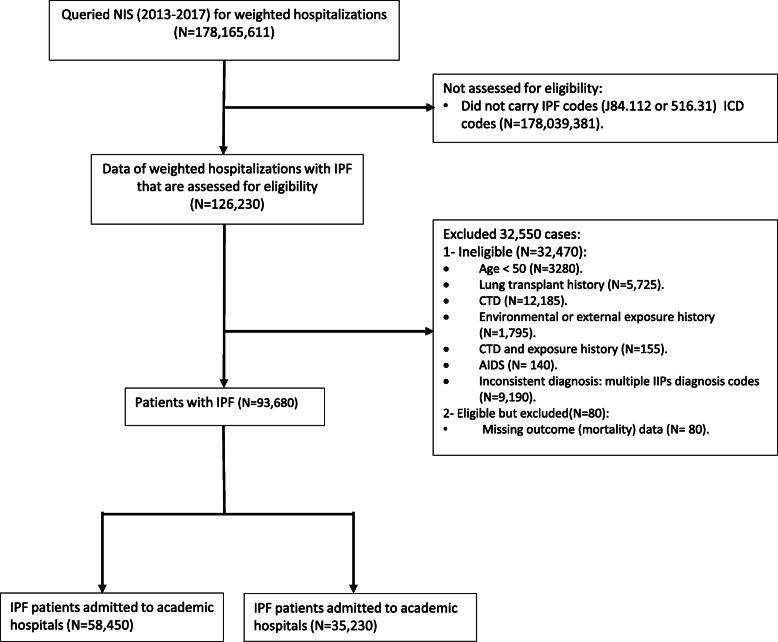
Hospitalization data was extracted from the National Inpatient Sample (NIS) for subjects with an international classification of disease code for IPF. In-hospital mortality stratified by hospital setting (academic versus non-academic) was the primary outcome of interest, with secondary analyses performed for subgroups with and without respiratory failure and requiring mechanical ventilation. Predictors of mortality were then assessed.
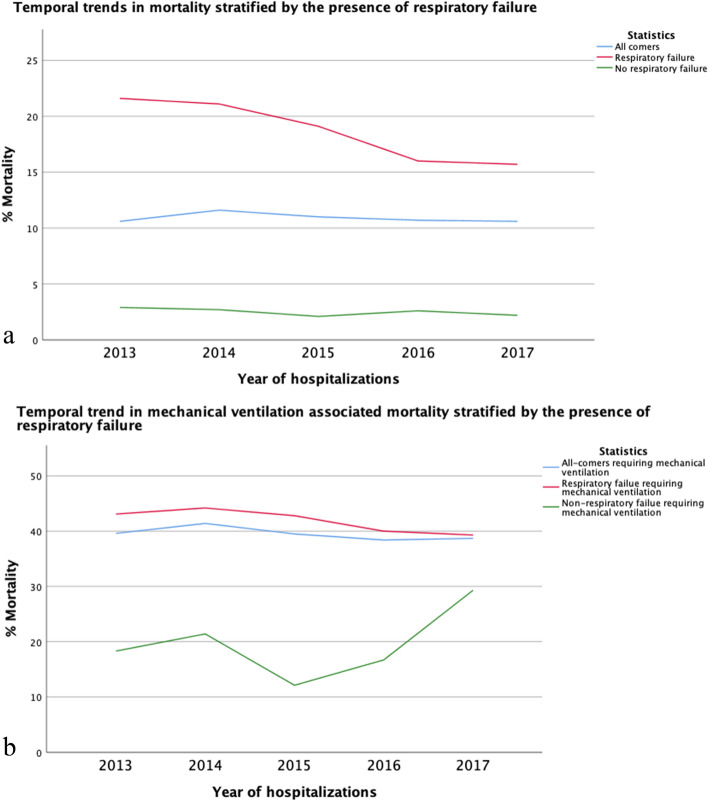
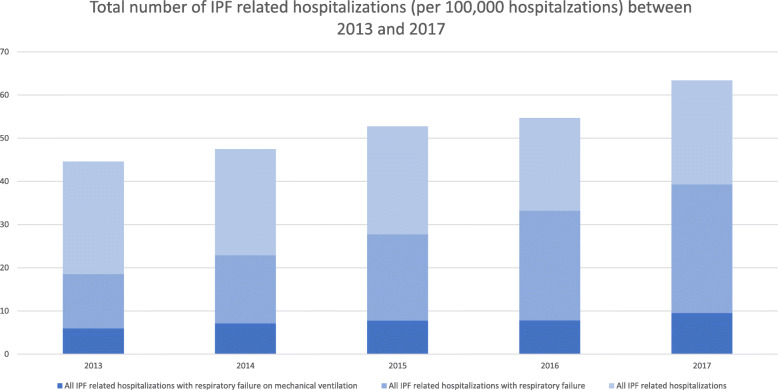
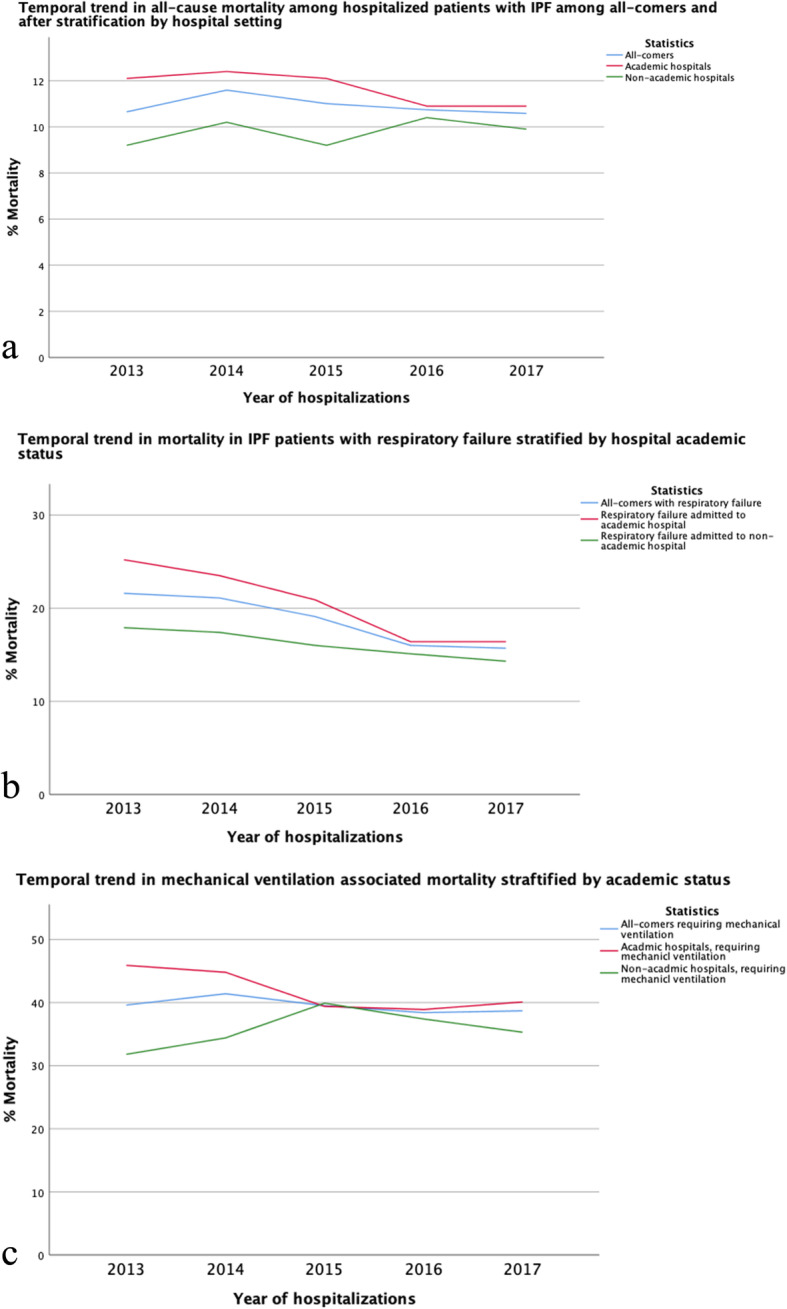
Among 93,680 patients with IPF requiring hospitalization, 58,450 (62.4%) were admitted to academic institutions. In-hospital mortality decreased significantly in those admitted to an academic hospital (p < 0.001) but remained unchanged in patients admitted to a non-academic hospital. A plateau in-hospital mortality was observed among all hospitalized patients (p = 0.12), with a significant decrease observed for patients with admitted respiratory failure (p < 0.001) and those placed on mechanic ventilation (p < 0.001).
In-hospital mortality decreased significantly for patients with IPF admitted to an academic hospital, suggesting that management strategies may differ by hospital setting. Mortality among those with respiratory failure and those requiring mechanical ventilation has dropped significantly. Our findings may underscore the importance of promoting early referral to an academic institution and adherence to international treatment guidelines.
特发性肺纤维化(IPF)是一种严重的疾病,其特征是肺功能进行性下降和早期死亡。虽然早期准确诊断对IPF治疗至关重要,但评估医院学术地位对IPF相关死亡率影响的数据仍然有限。在此,我们研究了2013年至2017年IPF患者的院内死亡率趋势。我们假设IPF的院内死亡率会受到医院学术环境的影响。
从国家住院样本(NIS)中提取患有IPF国际疾病分类代码的受试者的住院数据。按医院环境(学术性与非学术性)分层的院内死亡率是主要关注结果,对有和无呼吸衰竭以及需要机械通气的亚组进行了二次分析。然后评估死亡率的预测因素。
在93680例需要住院治疗的IPF患者中,58450例(62.4%)入住学术机构。入住学术医院的患者院内死亡率显著下降(p<0.001),但入住非学术医院的患者死亡率保持不变。在所有住院患者中观察到院内死亡率呈平稳状态(p = 0.12),而有呼吸衰竭的患者(p<0.001)和接受机械通气的患者(p<0.001)死亡率显著下降。
入住学术医院的IPF患者院内死亡率显著下降,这表明管理策略可能因医院环境而异。呼吸衰竭患者和需要机械通气患者的死亡率显著下降。我们的研究结果可能强调了促进早期转诊至学术机构以及遵循国际治疗指南的重要性。