Department of Emergency Medicine, Wake Forest School of Medicine (WFSOM), Winston-Salem, NC; Department of Biostatistics and Data Science, WFSOM, Winston-Salem, NC.
Department of Emergency Medicine, Wake Forest School of Medicine (WFSOM), Winston-Salem, NC.
Am Heart J. 2021 Feb;232:125-136. doi: 10.1016/j.ahj.2020.11.005. Epub 2020 Nov 6.
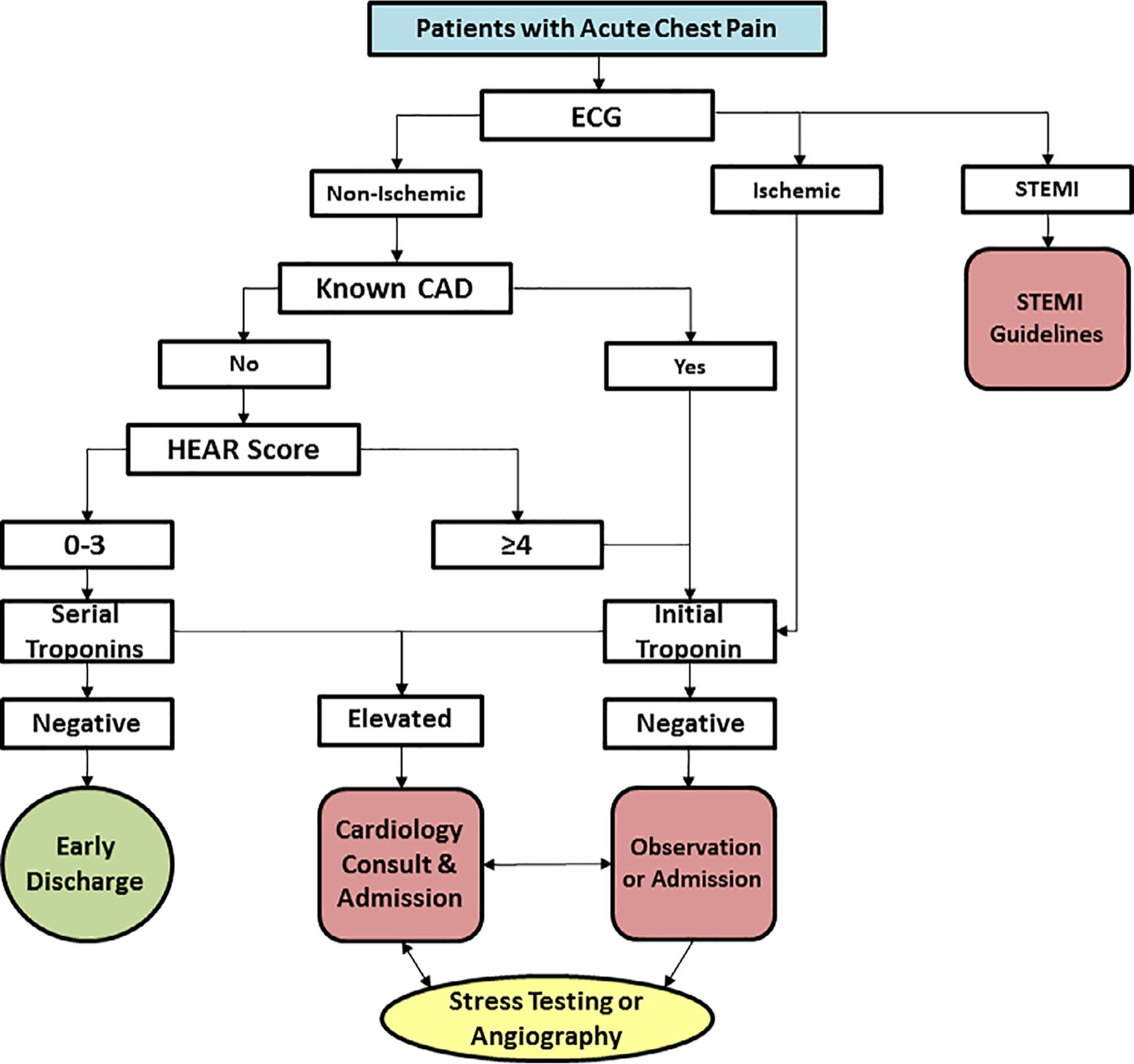
The HEART Pathway is an accelerated diagnostic protocol for Emergency Department patients with possible acute coronary syndrome. The objective was to compare the safety and effectiveness of the HEART Pathway among women vs men and whites vs non-whites.
A subgroup analysis of the HEART Pathway Implementation Study was conducted. Adults with chest pain were accrued from November 2013 to January 2016 from 3 Emergency Departments in North Carolina. The primary outcomes were death and myocardial infarction (MI) and hospitalization rates at 30 days. Logistic regression evaluated for interactions of accelerated diagnostic protocol implementation with sex or race and changes in outcomes within subgroups.
A total of 8,474 patients were accrued, of which 53.6% were female and 34.0% were non-white. The HEART Pathway identified 32.6% of females as low-risk vs 28.5% of males (P = 002) and 35.6% of non-whites as low-risk vs 28.0% of whites (P < .0001). Among low-risk patients, death or MI at 30 days occurred in 0.4% of females vs 0.5% of males (P = .70) and 0.5% of non-whites vs 0.3% of whites (P = .69). Hospitalization at 30 days was reduced by 6.6% in females (aOR: 0.74, 95% CI: 0.64-0.85), 5.1% in males (aOR: 0.87, 95% CI: 0.75-1.02), 8.6% in non-whites (aOR: 0.72, 95% CI: 0.60-0.86), and 4.5% in whites (aOR: 0.83, 95% CI: 0.73-0.94). Interactions were not significant.
Women and non-whites are more likely to be classified as low-risk by the HEART Pathway. HEART Pathway implementation is associated with decreased hospitalizations and a very low death and MI rate among low-risk patients regardless of sex or race.
HEART 路径是一种用于急诊科可能患有急性冠状动脉综合征的患者的加速诊断方案。目的是比较女性与男性、白种人与非白种人之间 HEART 路径的安全性和有效性。
对 HEART 路径实施研究进行了亚组分析。2013 年 11 月至 2016 年 1 月,从北卡罗来纳州的 3 个急诊科招募了胸痛的成年人。主要结局是 30 天内的死亡、心肌梗死(MI)和住院率。逻辑回归评估了加速诊断方案实施与性别或种族的相互作用以及亚组内结局的变化。
共纳入 8474 例患者,其中 53.6%为女性,34.0%为非白人。HEART 路径将 32.6%的女性患者归类为低危,而 28.5%的男性患者归类为低危(P=0.02),35.6%的非白人患者归类为低危,而 28.0%的白人患者归类为低危(P<.0001)。在低危患者中,30 天内死亡或 MI 的发生率为 0.4%的女性患者与 0.5%的男性患者(P=0.70)和 0.5%的非白人患者与 0.3%的白人患者(P=0.69)。30 天住院率降低了 6.6%的女性患者(OR:0.74,95%CI:0.64-0.85),5.1%的男性患者(OR:0.87,95%CI:0.75-1.02),8.6%的非白人患者(OR:0.72,95%CI:0.60-0.86)和 4.5%的白人患者(OR:0.83,95%CI:0.73-0.94)。交互作用不显著。
女性和非白人更有可能通过 HEART 路径被归类为低危。无论性别或种族如何,HEART 路径的实施与低危患者的住院率降低以及非常低的死亡和 MI 发生率相关。