Center for Pharmacoepidemiology Research and Training, Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania.
Center for Clinical Epidemiology and Biostatistics, Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania.
Kidney360. 2020 Jul 30;1(7):604-613. doi: 10.34067/kid.0001432020.
Nonsteroidal anti-inflammatory drugs (NSAIDS) are increasingly important alternatives to opioids for analgesia during hospitalization as health systems implement opioid-minimization initiatives. Increasing NSAID use may increase AKI rates, particularly in patients with predisposing risk factors. Inconclusive data in outpatient populations suggests that NSAID nephrotoxicity is magnified by renin-angiotensin system inhibitors (RAS-I). No studies have tested this in hospitalized patients.
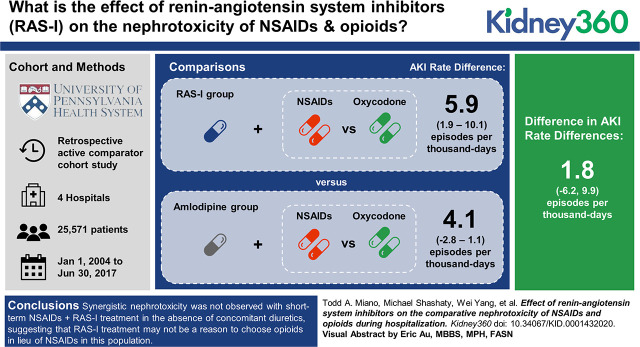
Retrospective, active-comparator cohort study of patients admitted to four hospitals in Philadelphia, Pennsylvania. To minimize confounding by indication, NSAIDs were compared to oxycodone, and RAS-I were compared to amlodipine. We tested synergistic NSAID+RAS-I nephrotoxicity by comparing the difference in AKI rate between NSAID versus oxycodone in patients treated with RAS-I to the difference in AKI rate between NSAID versus oxycodone in patients treated with amlodipine. In a secondary analysis, we restricted the cohort to patients with baseline diuretic treatment. AKI rates were adjusted for 71 baseline characteristics with inverse probability of treatment-weighted Poisson regression.
The analysis included 25,571 patients who received a median of 2.4 days of analgesia. The overall AKI rate was 23.6 per 1000 days. The rate difference (RD) for NSAID versus oxycodone in patients treated with amlodipine was 4.1 per 1000 days (95% CI, -2.8 to 11.1), and the rate difference for NSAID versus oxycodone in patients treated with RAS-I was 5.9 per 1000 days (95% CI, 1.9 to 10.1), resulting in a nonsignificant interaction estimate: 1.85 excess AKI events per 1000 days (95% CI, -6.23 to 9.92). Analysis in patients treated with diuretics produced a higher, albeit nonsignificant, interaction estimate: 9.89 excess AKI events per 1000 days (95% CI, -5.04 to 24.83).
Synergistic nephrotoxicity was not observed with short-term NSAID+RAS-I treatment in the absence of concomitant diuretics, suggesting that RAS-I treatment may not be a reason to choose opioids in lieu of NSAIDs in this population. Synergistic nephrotoxicity cannot be ruled out in patients treated with diuretics.
随着卫生系统实施阿片类药物最小化计划,非甾体抗炎药(NSAIDs)作为住院期间镇痛的替代药物,其重要性日益增加。增加 NSAID 的使用可能会增加急性肾损伤(AKI)的发生率,尤其是在有易感危险因素的患者中。在门诊人群中尚无定论的数据表明,肾素-血管紧张素系统抑制剂(RAS-I)会放大 NSAID 的肾毒性。没有研究在住院患者中对此进行过测试。
这是一项在宾夕法尼亚州费城的四家医院进行的回顾性、活性对照队列研究。为了最大限度地减少指示性混杂,将 NSAIDs 与羟考酮进行比较,将 RAS-I 与氨氯地平进行比较。我们通过比较 NSAID+RAS-I 治疗组与 NSAID+氨氯地平治疗组之间 AKI 发生率的差异,来测试 NSAID+RAS-I 治疗组与 NSAID+羟考酮治疗组之间 AKI 发生率的差异,以此来检验 NSAID+RAS-I 的协同肾毒性。在二次分析中,我们将队列限制在基线接受利尿剂治疗的患者中。使用逆概率治疗加权泊松回归对 71 项基线特征进行 AKI 发生率调整。
该分析共纳入 25571 名接受中位数为 2.4 天镇痛治疗的患者。总的 AKI 发生率为 23.6/1000 天。在接受氨氯地平治疗的患者中,NSAID 与羟考酮的比值差(RD)为 4.1/1000 天(95%CI,-2.8 至 11.1),而在接受 RAS-I 治疗的患者中,NSAID 与羟考酮的比值差为 5.9/1000 天(95%CI,1.9 至 10.1),这导致无统计学意义的交互效应估计值:每 1000 天额外发生 AKI 事件 1.85 例(95%CI,-6.23 至 9.92)。在接受利尿剂治疗的患者中进行的分析产生了更高的交互效应估计值,但无统计学意义:每 1000 天额外发生 AKI 事件 9.89 例(95%CI,5.04 至 24.83)。
在没有同时使用利尿剂的情况下,短期 NSAID+RAS-I 治疗并未观察到协同肾毒性,这表明在该人群中,RAS-I 治疗可能不是替代 NSAIDs 选择阿片类药物的理由。在接受利尿剂治疗的患者中,不能排除协同肾毒性。